
“In times of deceit, telling the truth is a revolutionary act.” George Orwell
“You will know the truth and the truth will set you free.” John 8:32
There has always been a relationship between knowing the truth and being free – just as there has always been a relationship between being fooled by lies and being a slave to those who are telling the lies.
This article is a part of our series of articles exposing the truth about a war being raged against the rights of our children – a war using weapons such as propaganda and lies, toxic addictive drugs, trans sports cheating and state-sponsored child abuse to arrest the natural and normal development of our children. Our goal is to use scientific truth as our first line of defense to win this war against our children’s rights.
Our mission is to advocate for a Childrens Bill of Rights that address each of these weapons being used against them. These fundamental rights include the right to be told the scientific truth about the world they will grow up in. As just one example, they have a right to know that there are only two biological sexes – male and female – and that changing one’s name or taking toxic drugs will not change ones biological sex. Children have a right to a good education – free from political agendas. Children have a right to personal privacy that includes the right to single sex bathrooms and locker rooms. Gender confised children have a right to unbiased counseling to help them overcome their underlying mental health problems rather than masking those problems by taking a lifetime of toxic drugs.
Girls have a right to fair sports competition where they are not required to compete against boys who are at least 20% stronger than them. Most important, children have a fundamental right to be guided by their parents rather than being subjected to state-sponsored child abuse without the knowledge of their parents.
In this report, we will focus on the scientific truth and use the scientific method to expose one of the worst crimes ever committed against our kids and our democracy, namely the forced “social and medical transition” of gender confused children and the Washington law banning troubled children from getting the counseling they so desparately need.
The Difference between Real Science versus Fake Science
Real Science broadly speaking is the systematic study of events to determine relationships between various factors or variables. Relationships include statistical or non-random correlations and time-ordered causations. Sorting out these relationships requires determining, isolating and controlling variables. Claims in science are called models and hypotheses. Claims must be supported with independently verifiable evidence. While models and hypotheses based on models may be proposed and evidence gathered through experiments to support or refute a hypothesis, the default hypothesis, called the Null Hypothesis, is that there is no relationship between the variables.
The burden of proof is on the scientist to provide evidence to refute the Null Hypothesis and support their alternative hypothesis. Experiments should be repeatable so that other scientists can confirm the results.
Fake Science, including Transgenderism include unsupported statements made by so-called “experts” using undefined terms such as “gender identity” and badly designed experiments such as self-report surveys known to suffer from confirmational bias and “rigged” experiments used by drug companies in order to sell drugs and make billions of dollars in profits. Fake science is relevant to the rise of Transgenderism because nearly all of the claims made by those advocating Transgenderism are based on the results of fake science. Here we define Transgenderism to include the claim that it is possible to change a person’s gender or sex by changing their name, their pronouns and by taking a lifelong series of toxic drugs ranging from puberty blockers to cross sex hormones and or by cosmetically altering ones appearance through genital mutilation.
Seven Differences between Real Science versus Fake Science
In real science, the motive is to learn the truth. In fake science, the motive is greed. Fake science is driven to promote predetermined outcomes that make billions of dollars for corporations, such as drug companies, who will benefit from the press releases associated with the incorrect outcomes (also known as lies) of the fake science.
There are several tricks used by the con artists who create fake science One of the most common tricks is to cherry pick the data. This is done by selecting samples that do not represent the entire population. Alternately, subjected are improperly excluded to achieve the desired outcome. By contrast, in real science, the entire population is represented and all subjects must be included in the data set.
Another trick of fake science is to ignore the time order of events. For example, in more than 40 studies used to promote Transgenderism, suicidal attempts of subjects were blamed on “conversion therapy” counseling when in fact the suicide attempts occurred months and years BEFORE the counseling and it was the suicide attempts that led to the counseling, not the counseling that caused the suicide attempts. By contrast, in real science, time order of events is always taking into account.
Another trick of fake science is to fail to isolate variables. Effects due to one variable can then be attributed to a different variable. By contrast, real science analyzes and accounts for all major variables.
Another shocking attribute of fake science is making claims about studies that are not supported by the actual data. For example, fake scientists will often make claims of huge improvements in kids who are given Transgender drugs – and even issue press releases of their success. But even a casual examination of the actual data supports the exact opposite claim – that subjects not only got worse but some of the subjects even committed suicide or died from being given toxic drugs. By contrast, real science reports all outcomes accurately.
Another trick of fake science is to report only some of the data – or in many cases – to not report the data at all. Real science by contrast reports all of the data – even data that does not support their initial hypothesis.
Finally, fake science limits and censors debate by claiming that the “science is settled.” By contrast, in real science, debate is encouraged with the understanding that all claims and models are subject to change and expected to change as new data is provided. In real science, scientific knowledge evolves and advances through continual debate. Non-scientists mistakenly assume that this never-ending debate means that scientific truth is in doubt. Instead, what it really means is that scientific truth evolves over time as new data is provided. In short, scientific models are not stagnant and debate is a good and even essential component of real science.
Real science can be further divided into Hard sciences and Soft sciences
Hard sciences relevant to the subject of Child Development include Inorganic Chemistry, Organic Chemistry, Genetics, Exogenetics, Biology and Neurobiology. Hard sciences use objective variables which can be more accurately measured than subjective variables. Mathematical models are common to provide more control over the variables and thus conclusions are more reliable.
Soft sciences relevant to the subject of Child Development include Psychology, Medicine, Education and Child Counseling. Soft sciences use the process of collecting empirical data then use the a variety of methods to collect and analyze information. Because soft science experiments often use variables that are difficult to objectively measure, the results of soft science are much less reliable and more subject to debate than the results of hard sciences. The most common way to improve the reliablity of soft science is through the use of Random Control Trials (RCT). However Random Control Trials are rarely used in experiments involving adults and almost never used in experiments involving children. When they are used, it is common to find a very wide degree of statistical variation. Soft sciences are also much more subject to cultural, social, political and economic influences. Thus, soft sciences are less accurate than hard sciences. This does not mean that soft sciences are less important than hard sciences. Merely that one must be careful about drawing conclusions based on soft science claims and soft science evidence.
The best way to understand Child Development is by combining research from both Hard Science studies and Soft Science studies.

Genetic Differences between Human Males and Females
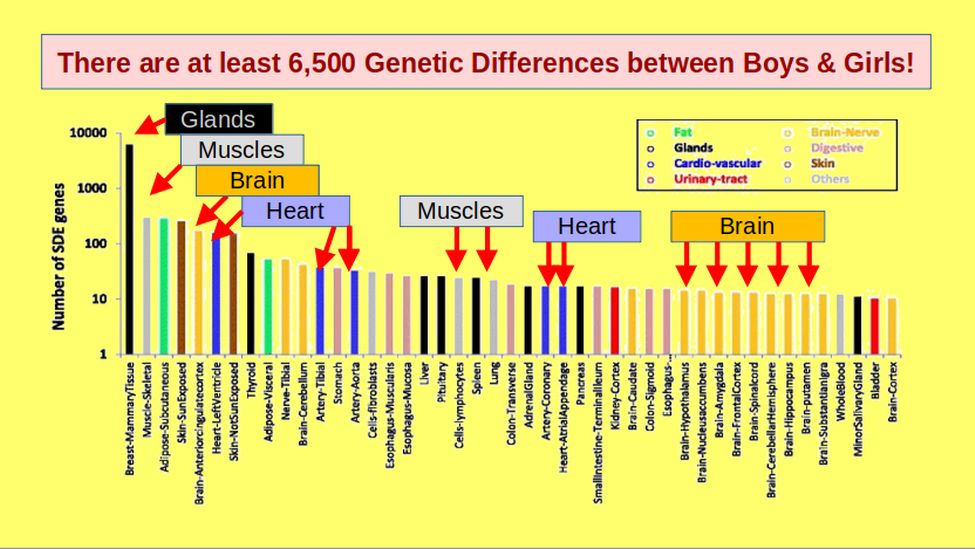
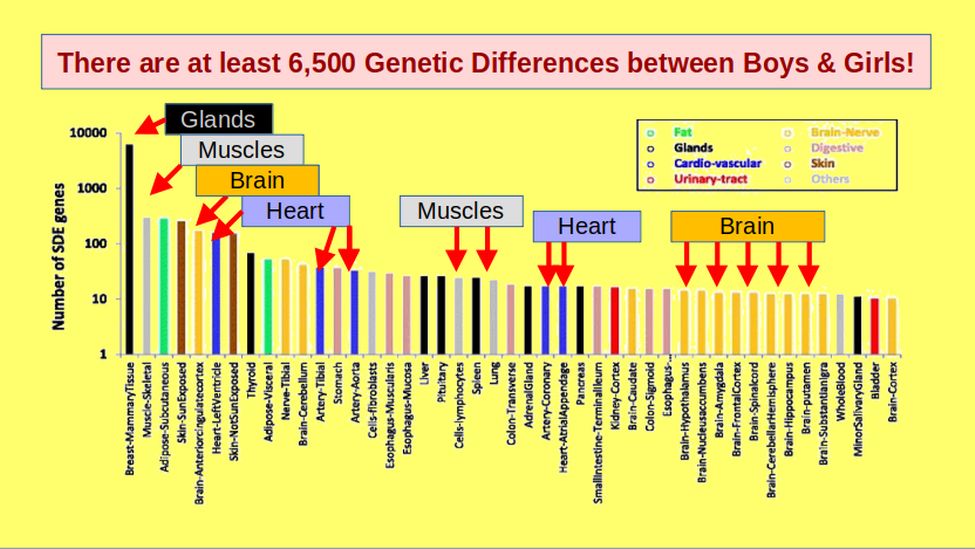
In terms of differences in the development of human males versus females, the hard science of Genetics confirms that there are more than 6,500 significant genetic differences between human males and females. Nearly all of these 6,500 variations are at the cellular level – meaning they affect nearly every cell in the body including every neuron in a person’s brain.
A 2017 study identified and analyzed differences between genetic markers linked to the human X or Y chromosomes. Here is a link to this study: https://bmcbiol.biomedcentral.com/articles/10.1186/s12915-017-0352-z
Over 30 different areas of the body are affected by these 6,500 differences.
Varying one or two hormones after a child is ten years old still leaves a biological male with 6,498 objectively measureable differences compared to a biological female. For example, the mitochondria in male cells have a higher metabolic rate than the mitochondria in female cells. This measurable difference appears within two days of conception. This is likely one of the reasons women live about 10 years longer than men. In addition, female brain development runs about three years ahead of male brain development.
Serotonin differences in the brain are only one of these 6500 genetic differences. Serotonin production is regulated by a particular group of genetic markers that act (are expressed) much differently in males and females. The serotonin levels in male brains is about ten times greater than in female brains. This is likely one of the reasons why girls are more sensitive to stress and why girls are more likely to suffer from Depression than boys.
Given these thousands of genetic differences between boys and girls, it is absurd to claim that giving kids a couple of drugs will be able to magically turn them into the opposite sex. From a standpoint of the hard science of genetics, giving a child any amount of drugs does not change them from a male to a female.
Soft science has also refuted the claims of Transgenderism. For example, advocates of Transgenderism have repeatedly claimed that society needs to affirm the gender identity of gender confused children in order to reduce the odds that the gender confused child will commit suicide. Numerous longterm studies of gender-affirmed versus gender-not-affirmed children have confirmed that the exact opposite is true – that affirming the gender of a gender-confused child and giving them drugs and surgery increases their risk of suicide. Instead, Soft Scientific studies have confirmed that gender-confused children nearly allows suffer from Adverse Childhood Events leading to serious mental health problems PRIOR to their gender confusion.
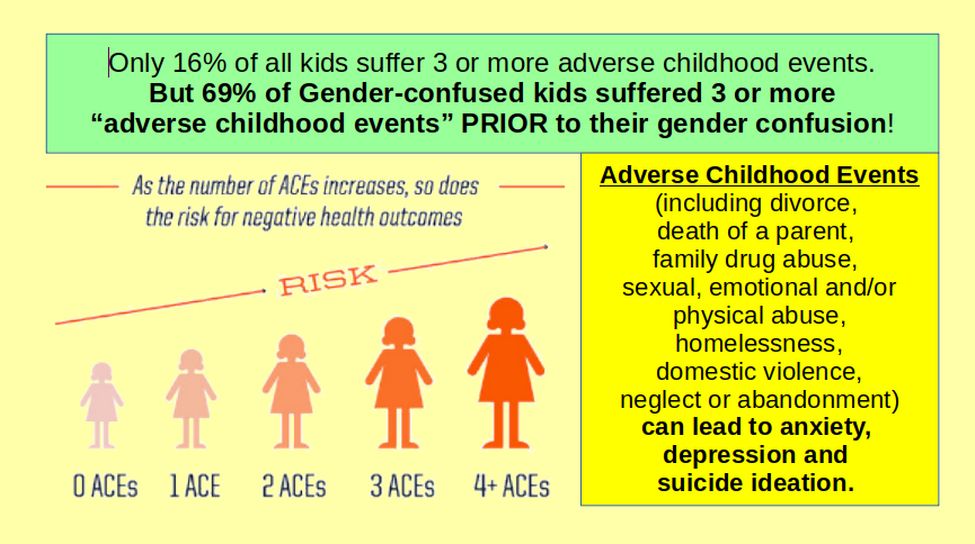
A 2021 Australia study found gender confused children had suffered an average of 5.5 adverse childhood events compared to 1.7 for the control group. Likely as a result of these ACEs, 86% of gender confused children suffered from at-risk attachment patterns compared to 18% for the control group. Here is a link to this study: https://www.frontiersin.org/journals/psychology/articles/10.3389/fpsyg.2020.582688/full
In addition, 88% of the gender confused group in this study suffered from a serious mental health problem.It should therefore be no surprise that most gender confused kids suffer from serious mental health problems PRIOR to their gender confusion. Gender confusion is therefore a symptom of underlying mental health problems – not a condition to be “fixed” with toxic drugs.
Children suffering from adverse events should be given counseling to help them cope with these events – not drugs to hide these events. Two forms of counseling (Cognitive Therapy and Interpersonal Therapy) have both been shown to reduce the risk of suicide. However, both of these forms of counseling have been banned in many “drug-only” states, including Washington state, by falsely labeling and legally defining them as “Conversion Therapy” simply because they do not affirm the so-called “gender identity” of the child and instead seek to help a gender-confused child address their underlying mental health problems.
A 20 year old battle between Counselors and Drug Pushers
Both the Title IX dispute and the Gender Counseling dispute are part of a larger 20 year battle between child development scientists and child mental health counselors versus so-called “Transgender advocates” and drug corporations that make billions of dollars getting kids addicted to toxic trangender affirming drugs. Drug corporations are so powerful that they also control major medical associations, the corrupt main stream media and the current leaders of the Democratic Party. Caught in the middle of this battle are parents, teachers and judges who have trouble figuring out which side of this debate to believe.
Because of the mountain of research confirm the harm of giving kids toxic drugs and the benefit of giving kids counseling, 25 states have already banned giving kids toxic trangender drugs.

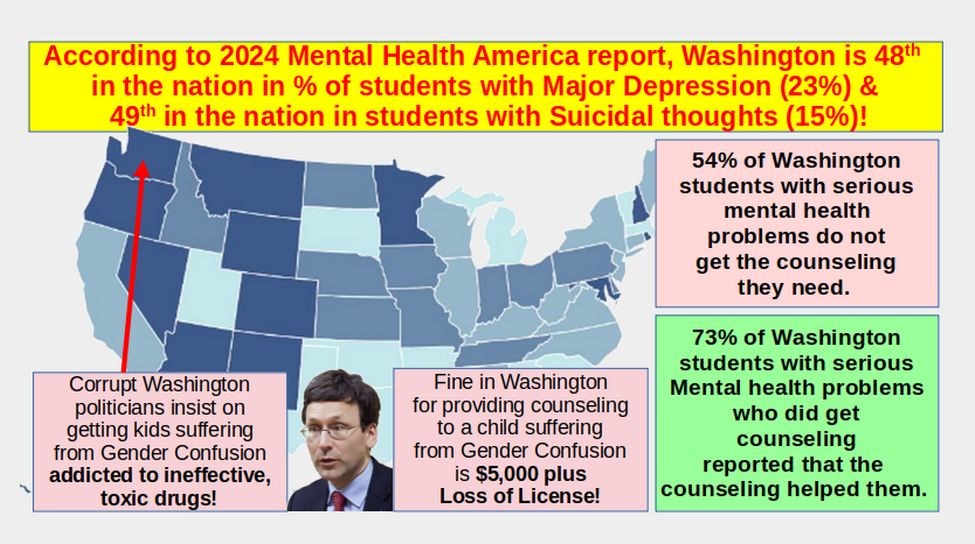
However, 23 states have banned giving Counseling to Gender Confused kids. This is because corrupt politicians like Bob Ferguson have falsely claimed that kids will kill themselves if you give them counseling instead of drugs. The “drugs only” states include Washington and Minnesota. The fine for providing a child with counseling to deal with their Gender Confusion in Washington is $5,000 plus loss of license!

Six years of banning counseling and requiring drugs has caused Washington state to fall to 48th in the nation in childhood mental health.
We need to ask ourselves - in the face of abundent evidence that drugs do not help kids while counseling does help kids - why any caring person would advocate for giving kids toxic drugs – and why any state legislature would pass a law prohibiting counseling and requiring toxic drugs?
Sadly, the reason Ferguson and Reykdal want to brainwash our kids into taking toxic drugs is to make billions of dollars for the drug companies that paid for their re-election campaigns.

Each child they convinced to take their toxic drugs makes a million dollars or more for their drug pushing bosses. Even worse, the people who get stuck paying the bill for these toxic drugs are the tax payers.
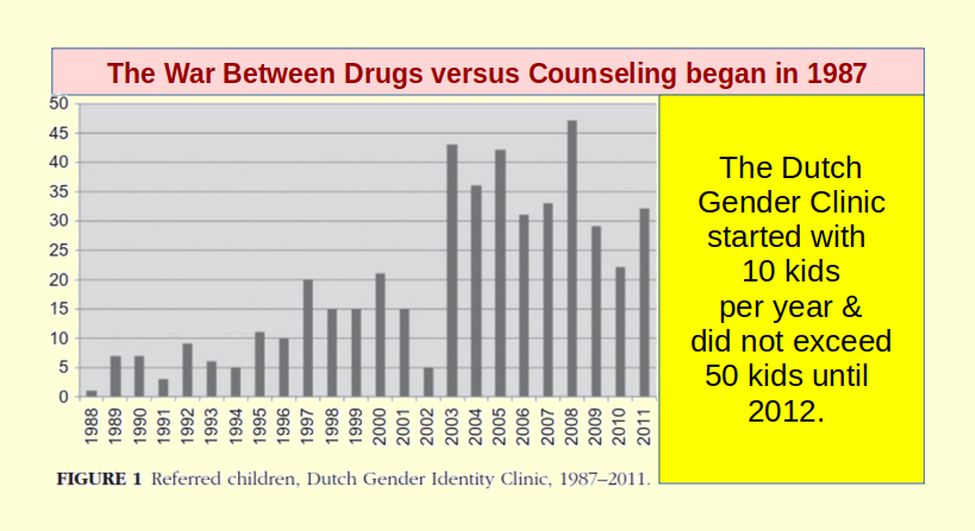
How the Battle between Drug Companies and Child Counselors began
The first attempt to treat gender confused children with a drug cocktail of cross sex hormones began in 1987 at the Dutch Gender Clinic, which mistakenly claimed that the drugs would be safe, effective and reversible. The average number of children treated each of the first 10 years was less than 10 and did not exceed 50 until after 2012. https://www.hbrs.no/wp-content/uploads/2017/05/Clinical-Management-of-Gender-Dysphoria-in-Children-and-Adolescents-The-Dutch-Approach.pdf
Up until the age of 14, children were only given counseling. At 14, they were given puberty blockers and then at age 16 transitioned into cross sex hormones. Here is a quote from a 2012 article about the Dutch Protocol: “Follow-up studies have demonstrated that only a small proportion of gender dysphoric children become transsexual at a later age… The proportions of persistence found in the initial studies were below 10% (for a review of the literature, see Zucker & Bradley, 1995)… Because most gender dysphoric children will not remain gender dysphoric through adolescence (Wallien & Cohen-Kettenis, 2008), we recommend that young children not make a social transition (a different name, referring to a boy as “her” instead of “him”) before the early stage of puberty… 14.”
In January 2023, three Transgender researchers published a 27 page review called “The Myth of Reliable Research in Pediatric Gender Medicine: A Critical Evaluation of the Dutch Studies – and research that has followed.” Here is a link to this article: https://www.tandfonline.com/doi/full/10.1080/0092623X.2022.2150346#abstract
This review explained how the original Dutch Protocol for “transitioning” gender confused children was not “safe” or “effective” or “reversible.” Instead, the Dutch Protocol, which involves giving gender confused kids toxic drugs, suffered from several serious flaws. Here is a quote from this 2023 review: “Two Dutch studies formed the foundation for the practice of youth medical gender transition. We demonstrate that this work is methodologically flawed and should have never been used in medical settings... We discuss the significant risk of harm that the Dutch research exposed, as well as the lack of applicability of the Dutch protocol to the currently escalating incidence of adolescent-onset, psychiatrically challenged youth. "Spin" problems—the tendency to present weak or negative results as certain and positive—continue to plague reports that originate from clinics that are actively administering hormonal and surgical interventions to youth. It is time for gender medicine to pay attention to the published objective systematic reviews and to the definable potential harms to these vulnerable youth.”
“A false narrative has taken root. It is that “gender-affirming” medical and surgical interventions for youth are as benign as aspirin, as well-studied as penicillin, and as essential to survival as insulin for childhood diabetes… This fallacious narrative has failed to withstand scientific scrutiny with public health authorities in Sweden, Finland, and most recently England doing a U-turn on pediatric gender transitions in the last 24 months.”
“Affirmative treatment” with hormones and surgery rapidly entered general clinical practice worldwide, without the necessary rigorous clinical research. Nor was it ever demonstrated that the benefits were substantial enough to outweigh the burden of lifelong dependence on medical interventions, infertility and sterility, and various physical health risks.”
“Several recent international systematic reviews of evidence have concluded that the practice of pediatric gender transition rests on very low quality evidence… Following these systematic reviews of evidence, three European countries—Sweden, Finland and England—have begun to recommend new and much more cautious treatment for gender dysphoric youth, which prioritize noninvasive psychosocial interventions (counseling) while sharply restricting the provision of hormones and surgery.”
“The two main Dutch studies in question, de Vries et al., 2011, and de Vries et al., 2014 (from here on, “the Dutch studies”) convincingly demonstrated that hormonal and surgical interventions can successfully change the phenotypical appearance of secondary sex characteristics of adolescents and young adults. What the studies failed to show, however, is that these physical changes resulted in meaningful psychological improvements significant enough to justify the adverse effects of the treatment—including the certainty of sterility.
In the case of the Dutch studies, we identified three major sources of bias, or systematic error, involving: (1) case selection (was retrospective and non-random); (2) measurement of outcomes; and (3) confounding of variables. One person was removed from the 70 person study because they died due to the intervention. Three others were removed because they developed severe diabetes and obesity. 15 others refused to continue with the study for unknown reasons. Thus, out of an initial study group of nearly 200 subjects, the study only reported on the 55 with the best outcome. Even with this level of cherry picking participants, there was very little improvement in mental health resulting from puberty blockers, cross sex hormones and surgery. The result was more likely to be due to the fact that as subjects get older, their mental health naturally improves. In addition, all the subjects received counseling as they went through medical transitioning and this also contributed to their improvement.
Genetic Differences affecting the Development of Boys and Girls
There are huge differences between the development of boys and girls. For example, the mitochondria in the cells of boys have a much higher basal metabolic rate than the mitochondria of girls. This difference appears within two days of conception. This is likely one of the reasons women live about 10 years longer than men. In addition, female brain development runs about three years ahead of male brain development. We also know that serotonin production is regulated by a particular group of genetic markers that act (are expressed) differently in males and females. The serotonin levels in male brains is about ten times greater than in female brains. This is likely one of the reasons why girls are more sensitive to stress and why girls are more likely to suffer from Depression than boys.
In 2017, a study was published that identified and analyzed differences between genetic markers linked to the human X or Y chromosomes. The study was called “The landscape of sex-differential transcriptome and its consequent selection in human adults.”
Here is a link to this study: https://bmcbiol.biomedcentral.com/articles/10.1186/s12915-017-0352-z
The study found that there are over 6,500 genes that are expressed differently (by producing different proteins) between the X and Y chromosomes. Over 1,000 of these genetic differences were related to breast mammillary glands. Hundreds were related to muscle development and many were related to brain development. Over 30 different areas of the body were affected by these 6,500 genetic differences:
Serotonin differences in the brain are only one of these 6500 genetic differences. Given these thousands of genetic differences between boys and girls, it is absurd to claim that giving kids a couple of drugs will be able to magically turn them into the opposite sex. But this is exactly what is promised to gender confused children by drug dealers and their accomplices. The first and perhaps worst batch of toxic drugs given to these troubled kids are called Puberty Blockers.
Adverse Effects of Puberty Blockers
The most common puberty blocker is called Lupron. It was approved by the FDA in 1993 based on a 2 year study of 22 children, several rats and several rabbits. Some rats developed cancerous tumors. In rabbits, it caused birth defects and abortions. In humans, it can cause convulsions in kids taking SSRIs. It can also cause wieght gain, obesity and mood swings. Here is what it looks like:
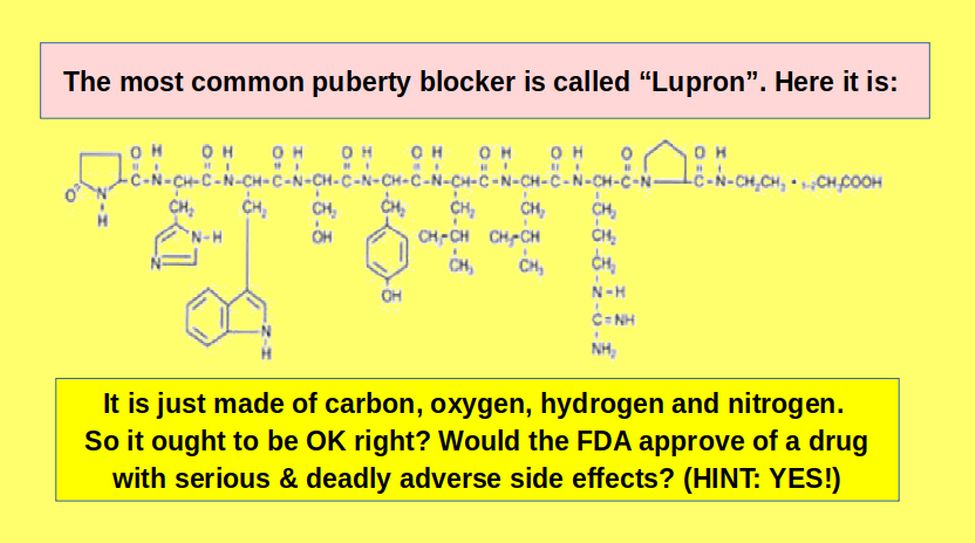
Here is a link to the 32 page FDA warning about this toxic drug. https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/020263s036lbl.pdf
The adverse effects of puberty blockers are serious and permanent. A 2010 drugmaker-sponsored a study looked of children who took Lupron from 1991 to 2009. The study reported that several of the 55 kids suffered serious side effects. 15 (27%) suffered mood swings and headaches. One person suffered a heart attack and died after two years of taking Lupron. https://s3.documentcloud.org/documents/3260007/Leuprolide-M90-516-Lee-Lupron-Study.pdf
More than 20,000 adverse-event reports have been filed with the FDA in the last decade. Women have reported to the FDA hundreds of cases of insomnia, depression, joint pain, and more than 100 cases of blurred vision. Among men who take Lupron, its label warns of increased risk of heart attacks, strokes and sudden death. https://www.statnews.com/2017/02/02/lupron-puberty-children-health-problems/comment-page-1/
In 1999, the FDA examined 6,000 adverse-event reports about Lupron filed by doctors, patients, and researchers. A court document that summarized the findings said it found “high prevalence rates for serious side effects” including depression, joint pain, and weakness, and noted similar effects in men and women with very different ailments suggested the drug was causing the problems rather than underlying medical conditions.
Lupron was back in the courtroom in 2008, when patient Karin Klein sued the drugmaker. Klein alleged that she was not adequately warned of the drug’s effects and after taking the drug as a teen for a uterine condition, developed degenerative disc disease, jaw-joint dysfunction, and bone thinning, court records show. According to a court record in her case, a report by Dr. John Gueriguian, a former FDA medical officer serving as an expert witness for Klein, said the drug causes “irreversible side effects and permanent severely disabling health problems.”
In a court document, one gynecologist said a salesperson told him he “could earn $100,000 annually” by treating women with Lupron. The settlement resulted in a corporate guilty plea for conspiracy to violate prescribing laws and one of the largest fines at the time, $875 million. https://www.justice.gov/archive/opa/pr/2001/October/513civ.htm
In 2017, the Center for Investigative Reporting revealed that the FDA had received more than 10,000 adverse event reports from women who were given Lupron off-label as children to help them grow taller. They reported thinning and brittle bones, teeth that shed enamel and cracked, degenerative spinal disks, painful joints, radical mood swings, seizures, migraines and suicidal thoughts. Some developed fibromyalgia. There were reports of fertility problems and cognitive issues. https://revealnews.org/article/women-say-drug-used-to-halt-puberty-has-ruined-their-lives/
Given that Lupron chemically castrates its recipients, diminishing gonadal hormone production entirely, we might expect a little more research and certainly more caution in prescribing this drug. This doesn’t appear to be the case, as tens of thousands of women, men, and even children are prescribed this drug every year and have been for decades.
The Internet is filled with stories of the devastation caused by Lupron and the research showing the mechanisms by which it induces damage. Despite the decades of anecdotal evidence of serious side effects and the bevy of lawsuits filed and/or settled there is very little quantitative research delineating the scope and severity of these side effects. It has been up to private individuals to document these side effects. For example, the Lupron Side Effects Survey was launched in 2013 to assess potential side effects across all organ systems. https://hormonesmatter.com/lupron-side-effects-survey-results-scope-severity-side-effects/
Hormones have receptors everywhere: it stands to reason then, if we deplete those hormones rapidly and continuously, there will be effects wherever those hormones play regulatory or modulatory roles. Of course, since estradiol, the primary hormone affected by Lupron, is critical to mitochondrial morphology, and thus mitochondrial energetics, anywhere there are high demands for energy, the nervous system, the heart, GI, musculature, we might anticipate a high degree of effects in those systems as well, especially with longer term use and as the damage accrues. Over 1000 Lupron victims completed the surveys. Estradiol affects insulin regulation and general metabolism, so it stands to reason that rapid weight gain was common (mild 19%, severe 26%). At least 10 women experienced a heart attack, 36 women developed mitral valve prolapse, 10 women developed blood clots in the leg and 8 women had pulmonary emboli.
Puberty Blocker Adverse Effect on Mood, Memory and Mental Health
The brain is a major target of and source for steroid hormones. The prefrontal cortex, hippocampus, and amygdala, responsible for regulating behavior, memory, and emotion, have high densities of estrogen receptors. Depleting estradiol thus can have a significant impact on these functions. More than 50% of women reported severe psychological disturbances ranging from depression and anxiety. 15% reported severe to life-threatening suicidality. 33% reported moderate to severe memory loss.
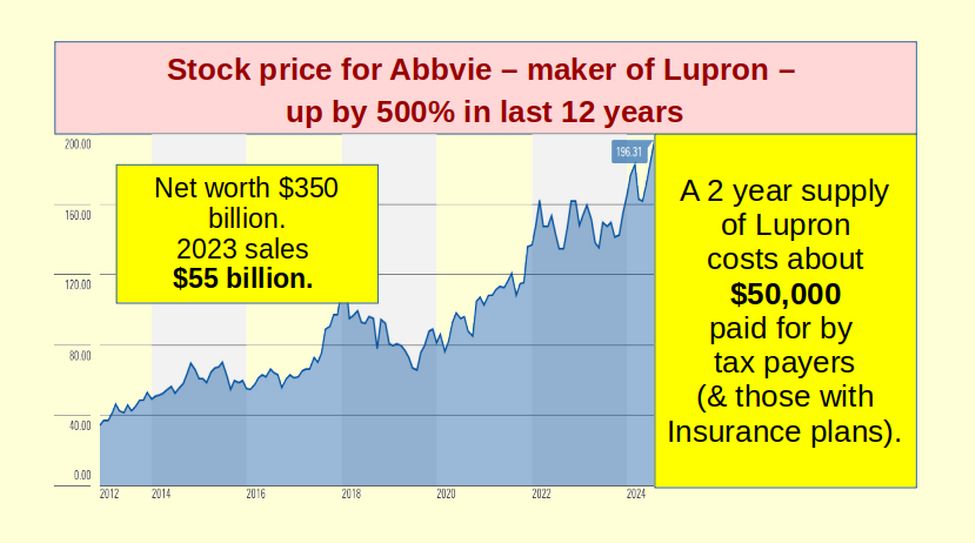
Lupron is very expensive — currently about $50,000 for two years of treatment. Transgenders may be on puberty blockers for 10 years so the total cost of just the blockers could reach $250,000 per person. Since 2012, the stock price of its maker, AbbVie, went from $40 to $200 a share – a 500% increase. AbbVie is worth $350 billion. 2023 revenue was $55 billion.
Adverse Effects of Cross Sex Hormones
The second batch of toxic drugs given to kids are very high does of cross sex hormones. While in the Dutch protocol, cross-sex hormones are started at 16 years, cross sex hormones in the US often start at age 12. It is assumed that cross-sex hormones will sterilize the victim of this blatant child abuse. Cross sex hormones begun in adolescence are likely to be administered for four to six decades. A recent article in the New England Journal of Medicine tracked 315 youths undergoing 2 years of gender affirming hormones (Chen 2023). Within 315 hormone treated youth there were 2 completed suicides. Curiously, this remarkably high suicide rate is not explored in the article. Several researchers have reported that cross- sex hormones increase the occurrence of various types of cardiovascular disease, including strokes, blood clots, and other acute cardiovascular events. Getahun, D., et al. (2018). Cross-sex Hormones and Acute Cardiovascular Events in Transgender Persons. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6636681/
The published evidence of adverse impact, coupled with the lack of data sufficient to reach a firm conclusion, make it irresponsible to assert that cross-sex hormones “are safe.”
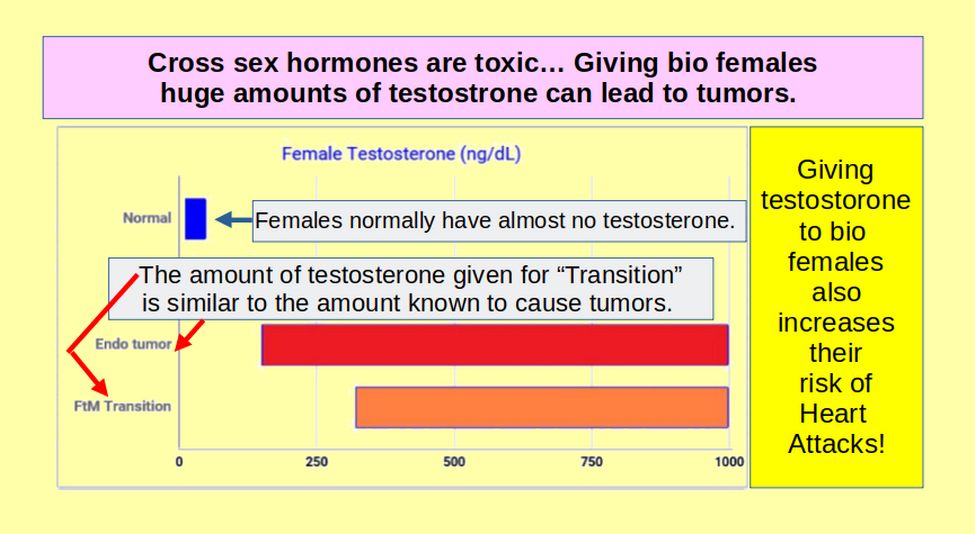
Danger of giving male hormones to bio females
Girls normally have almost no testosterone. So-called Gender Affirming Care (GAT) requires giving girls who want to be boys huge doses of testosterone to ultimately raise their levels of testosterone to 320 to 1000 ng/dL11 which is the same level as dangerous tumors for women.
A 2022 study of adverse drug reactions (ADRs) as part of gender affirming hormone therapies in France states that “our data show a previously unreported proportion of cases indicating cardiovascular ADRs in transgender men younger than 40 years… In transgender men (bio females) taking testosterone, all reported ADRs were cardiovascular events, with pulmonary embolism in 50% of cases” (Yelehe et al., 2022) "Adverse effects of gender-affirming hormonal therapy in transgender persons." Fundamental and Clinical Pharmacology. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9796635/
With respect to cardiovascular risk “Studies of transgender males (bio females) taking testosterone have shown up to a nearly 5-fold increased risk of heart attacks relative to females not receiving testosterone” (Laidlaw et al.,2021; “Erythrocytosis in a Large Cohort of Trans Men Using Testosterone” The Journal of Clinical Endocrinology & Metabolism, https://doi.org/10.1210/clinem/dgab514
Regarding Testostorone abuse, the labeling reads "Testosterone has been subject to abuse... steroid abuse can lead to serious cardiovascular and psychiatric adverse reactions...Abuse of testosterone is seen in male and female adults and adolescents… There have been reports of venous thromboembolic events [blood clots], including deep vein thrombosis (DVT) [blood clot of the extremity such as pulmonary embolism (PE) [blood clot of the lung which may be deadly… There are also serious concerns regarding liver dysfunction: “Prolonged use of high doses of androgens ... has been associated with development of tumors, cancer and life-threatening liver problems” (Actavis Pharma, 2018).
Research has shown that steroid abuse predisposes individuals to mood disorders, psychosis, and psychiatric disorders. The most prominent psychiatric features associated with testosterone abuse are manic-like presentations defined by irritability, aggressiveness, euphoria, grandiose beliefs, hyperactivity, and reckless or dangerous behavior. Other psychiatric presentations include the development of acute psychoses, depression and acute confusional/delirious states. (Hall, 20005) "Psychiatric Complications of Anabolic Steroid Abuse". Psychosomatics 46:4, July-August 2005
Danger of giving female hormones to bio males
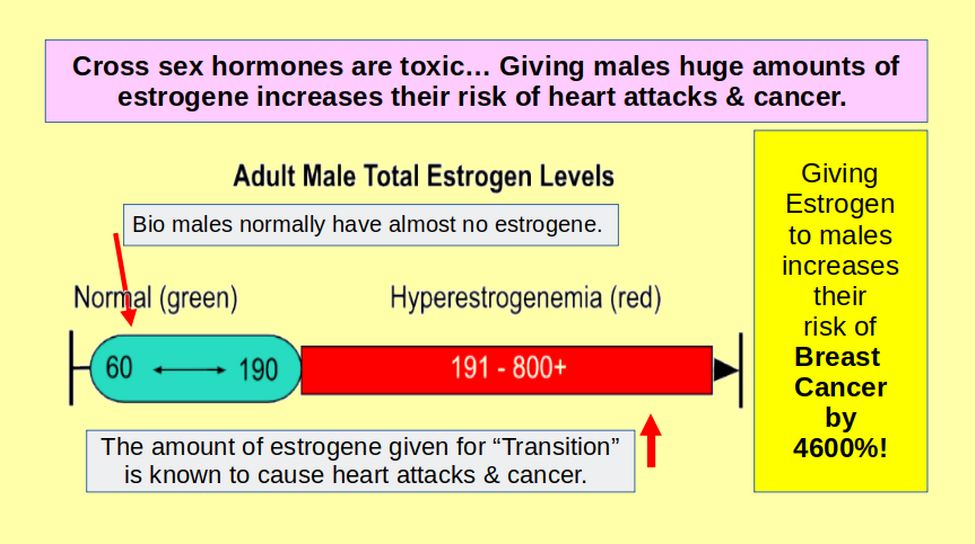
Estradiol is a type of estrogen. The normal adult male estradiol range is 60 pg/mL. In gender affirmative therapy, the medical condition of hyperestrogenemia is being deliberately, medically induced by the off-label use of high doses of Estradiol. Estradiol levels are raised to 200 pg/mL, three times above the normal range in an attempt to increase male breast tissue development. Long-term consequences of hyperestrogenemia include increased risk of heart attacks and death due to a five-fold increase in cardiovascular disease (Irwig, 2018)."Cardiovascular health in transgender people." Rev Endocr Metab Disord. 2018;19(3):243–251
Giving bio males female hormones also greatly increases the risk of breast cancer. Breast cancer is a relatively uncommon in males. However, the risk of a male developing breast cancer has been shown to be 46 times higher (4,600 percent) with high dose estrogen (Christel et al., 2019). "Breast cancer risk in transgender people receiving hormone treatment: nationwide cohort study in the Netherlands" BMJ 2019; 365 https://www.bmj.com/content/bmj/365/bmj.l1652.full.pdf
Change in Gender Confusion from Autistic Boys to Depressed Girls
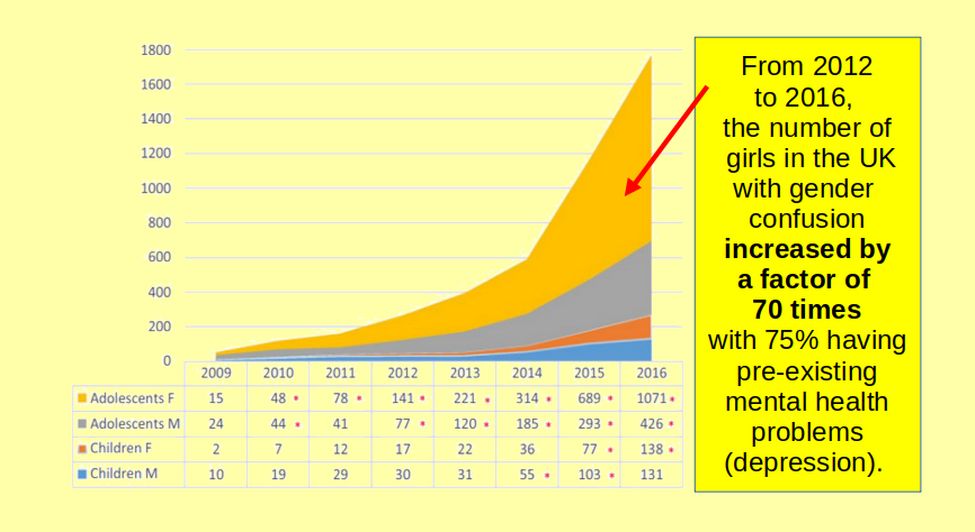
Around 2014, the presentation of gender dysphoria in the Western world sharply shifted, from childhood-onset that skewed toward males, to adolescent-onset with a preponderance of females with mental health problems. Finnish researchers saw a new pattern of “severe psychopathology preceding onset of gender dysphoria,” with 75% already in treatment for other psychiatric issues before their gender dysphoria emerged. The number of females presenting with gender dysphoria in the UK increased by a factor of 70 in just 4 years. https://pubmed.ncbi.nlm.nih.gov/29696550/
2018 Washington passes a Gender Counseling Ban
Since 2018, Washington is one of several states that have banned counselors from speaking with gender confused children about the underlying causes of their gender confusion. As insane as it sounds, Senate Bill 5722 requires licensed counselors in Washington to promote state-sponsored child abuse of giving gender confused children toxic drugs.
This crazy law is an attack on our free speech rights under the First Amendment. It is also an attack on the scientific method as science requires the ability to consider all points of view – and not be limited to only the official dogma. Finally, this new law is an attack on at-risk children – because it forces children to go down a deadly drug path and prevents them from having access to counseling that might help them overcome their mental health problems.
For the past eight years, Bob Ferguson and his accomplices have been telling several Big Lies – including his claim that a federal law called Title IX requires us to allow boys in the girls bathroom and allow boys to compete in girls sports. The driving force behind this law is not a concern for Trangender children but the extreme greed of the drug industry that stands to make billions of dollars in profits by getting vulnerable children addicted to toxic transgender drugs.
Even worse, Ferguson claimed that if a teacher spoke out against his new rules, they would be “risking the lives of Transgender kids” and would therefore be guilty of committing a crime so dangerous that they could lose their teaching job. Any child who spoke out could be kicked out of school – and any parent who dared to speak out could lose their children. In short, no one is allowed to speak out against the Ferguson Drug Cartel.
Yet there is a simple reason that giving gender confused kids toxic drugs to solve their problems is doomed to failure while providing children with counseling offers at least the possibility of success. The fact is that each child is unique. This is why child counseling begins by asking each child about their past experiences and their feelings about those experiences. It is the best way to get at the underlying causes of child’s problems. By contrast, giving troubled children drugs treats all children as if they are the same. It relies on the desire of parents for a simple “magic bullet” solution. It is the con game of drug peddling snakeoil salesmen and corrupt politicans like Bob Ferguson and Chris Reykdal.
Our task in this report is to expose lies of Ferguson and Reykdal and help bring the truth to the light of day. To do this, we will review scientific studies on the harm of transgender drugs increasing the risk of suicide and the benefit of child counseling reducing the risk of suicide.
Scientific studies on the harm of transgender drugs increasing the risk of suicide
For the past eight years, Bob Ferguson and his accomplices have based their revision of Title IX and their ban on child counseling on the claim that if we do not give gender confused kids toxic drugs to “affirm” their desired gender, 51% of these kids will attempt to kill themselves. Ferguson began filing more than a dozen Transgender Drug Promotion Amicus briefs as far back as 2016. One of his latest briefs was filed with the US Supreme Court on July 6 2023, in a case called Tingley versus Ferguson. Here is a link to Ferguson’s brief: https://www.supremecourt.gov/DocketPDF/22/22-942/270446/20230705162425629_zzz%20CENTERED%20FOR%20FILING.pdf
Tingley is a counselor in Washington state who claims that the Washington law prohibiting counseling of gender confused children violates his First Amendment rights. The draconian law imposed a fine of $5,000 and loss of license for any licensed counselor wanting to provide troubled kids with counseling. We will focus on the “fake science” cases provided by Bob Ferguson in his 48 page opposition brief as well as real scientific studies not provided by Ferguson confirming how harmful it is to give drugs to troubled children and how beneficial it is to give kids counseling instead.
Beginning on page 14, Ferguson provides a series of studies to support his claim that “Conversion Therapy” (which is Ferguson’s term for child counseling) is “widely discredited” (when in fact, nearly all real studies have discredited giving kids toxic gender drugs and instead recommend providing troubled children with counseling). The first study was a 2009 report by the American Psychological Association called “Task Force on Appropriate Therapeutic Responses to Sexual Orientation.” Apparently, Ferguson fails to realize that many professional groups like the APA and MDA have been completely taken over by the Drug Industry. The second study was a 2023 report by the Department of Health and Human Services called “Moving Beyond Change Efforts.” DHHS, like many other federal agencies, is also completely controlled by Drug Corporations.
Ferguson claims that “Conversion therapy puts minors at risk of serious, long-lasting harms, including increased risks of suicide and depression.” To support this claim he refers to pages 26 to 30 of te DHHS report. These 5 pages include links to 15 studies. Most of these studies are behind paywalls. One was just a Biden administration policy that has been rejected by several federal courts. Others simply listed conclusions without reporting the data on which the conclusions are based. Here we will look at four studies which are not behind paywalls and that included the data so we can see how the Drug Industry manipulates data to draw conclusions that are the exact opposite of what the data really shows.
2015 self report survey of 3405 Transgender people
One of the studies is a 2015 self report survey of 3405 Transgender people, 89 of whom were given Transgender “Puberty Suppression” drugs. Here is a link to this survey: https://publications.aap.org/pediatrics/article/145/2/e20191725/68259/Pubertal-Suppression-for-Transgender-Youth-and
Here is the actual table of outcomes in the study:
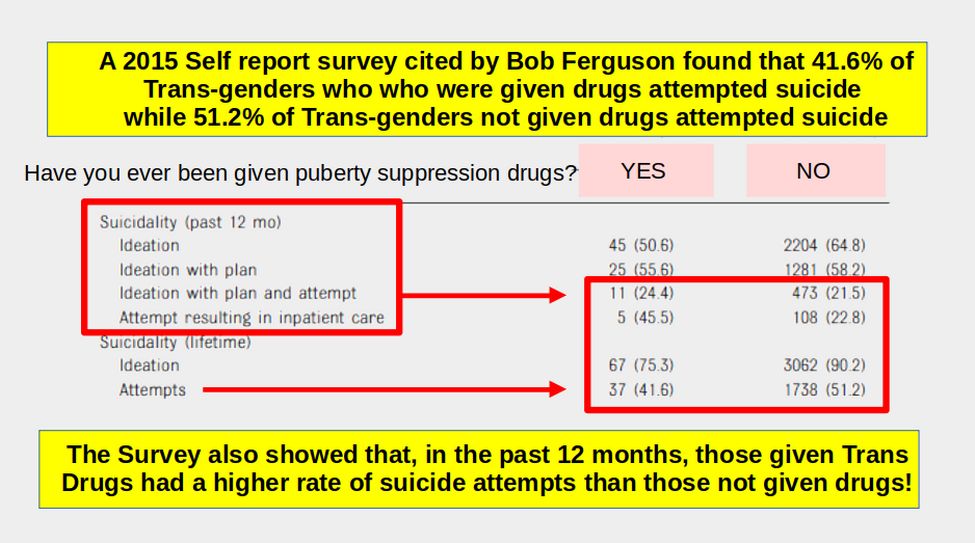
The last row shows that 41.6% of the Trans people given drugs had Lifetime Suicide attempts and 51.2% of the Trans people not given drugs had Lifetime Suicide attempts. But much more important, 45.5% of those given gender mutilation drugs attempted to commit suicide in the previous 12 months with the attempt putting them in the hospital. Meanwhile, only 22.8% of those not given gender mutilation drugs had a suicide attempt that put them in the hospital.
To understand how both of these “facts” can be true, all we need to do is look at the average age of those given drugs versus those not given drugs. Here is Table 1 showing the claimed age difference:
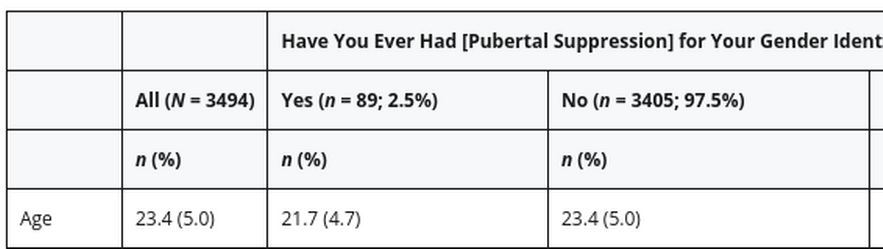
Note that the average age for the entire sample was 23.4 which was also the average age for those not given drugs. Meanwhile, the average age for those given drugs was only 21.7. But a huge flaw of this online self report survey was that the minimum age to take the survey was 18. Also, the most common response for age was 18 – which clearly indicates a non-random response. In fact, it is certain that many 16 and 17 year olds took the survey and checked the 18 box because there was no 16 ot 17 box. These younger people were very likely to be in the group given drugs since government payment for those drugs in the US was only available since passage of the Affordable Care Act 4 years before the survey. When we adjust for this fact, the actual age of those given Trans drugs is about 20.
In addition, it is known that suicide risk is much higher, Trans or Not, after the onset of puberty. We will assume puberty starts at age 12. Thus the Trans Drug group had a Suicide “Lifetime” of 20 minus 12 equals 8 years while the Trans No Drug group had a Suicide “Lifetime” of 23.4 minus 12 equals 11.4 years. Therefore, the Trans Drug group Suicide Attempts Percent per year was 41.6% divided by 8 years equals 5.2% percent per year. Trans No Drug group Suicide Attempts Percent per year was 51.2% divided by 11.4 years equals 4.5% per year.
Combining this fact with the fact that in the previous 12 months before the survey, the Trans Drug group had twice as many suicide attempts as the Trans No Drug group, it becomes obvious that giving drugs to transgender youth increases their rate of suicide – for the equally obvious reason that Trans drugs do not deal with the underlying mental health problems like Depression that led to the Gender Confusion in the first place. In short, the data from this study leads to the opposite of the claim made by Bob Ferguson and his accomplices.
What caring, rational person would advocate spending hundreds of millions of dollars giving tens of thousands of minors toxic gender drugs when the result of giving them those drugs results in a huge increase in suicide attempts that result in hospitalization?
To promote giving kids toxic drugs, Ferguson blatantly lied to the federal Court. But he did not merely lie to the Court, he lied to the American people, including millions of parents and children, about a gender drug policy that is currently harming thousands of children and costing the tax payers billions of dollars. In short, this may be one of the worst crimes Bob Ferguson has ever committed. The voters need to know about this crime because Ferguson is now running for Governor here in Washington. What the 2015 survey really confirmed was that transgenderism is not about “being born in the wrong body.” Instead, it is a symptom of an underlying mental health problem. The solution to this problem is to provide the child with counseling to address the underlying mental health problem – not giving the child toxic drugs to mask or ignore the mental health problem.
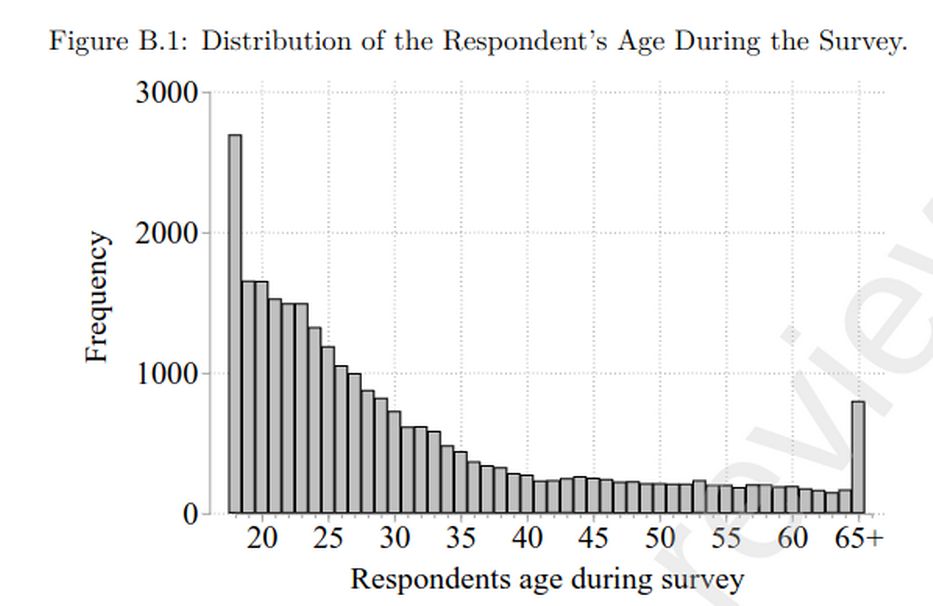
Second 2015 self report survey of Transgender people
The second study using the same data set as the first study is a 2023 study called “Conversion Therapy, Suicidality, and Running Away.” Here is a link to this study: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4180724
Despite being 76 pages long, this study failed to include the underlying data on which its conclusions were based. What it did include was a graph that confirm the age distribution of subjects in the 2015 survey. This graph confirms that age 18 was the most common response and thus the survey included kids age 16 and 17 just claiming they were 18:
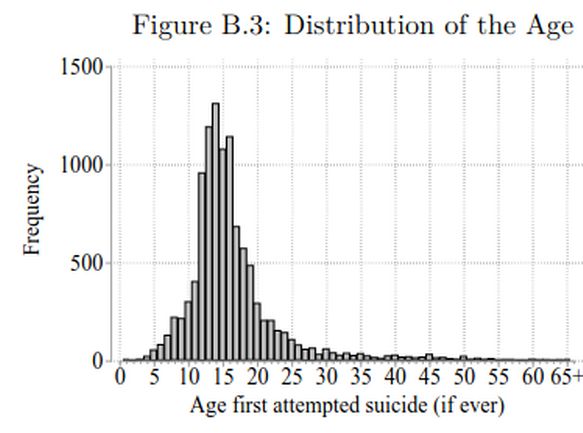
It also includes a graph of when subjects first attempted suicide which peaks at about age 14.
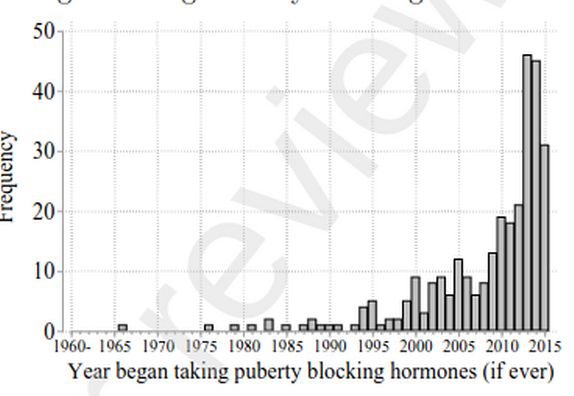
It also includes a graph of when pubery blocking hormones first became popular which was about 2014.
Third 2015 self report survey of Transgender people
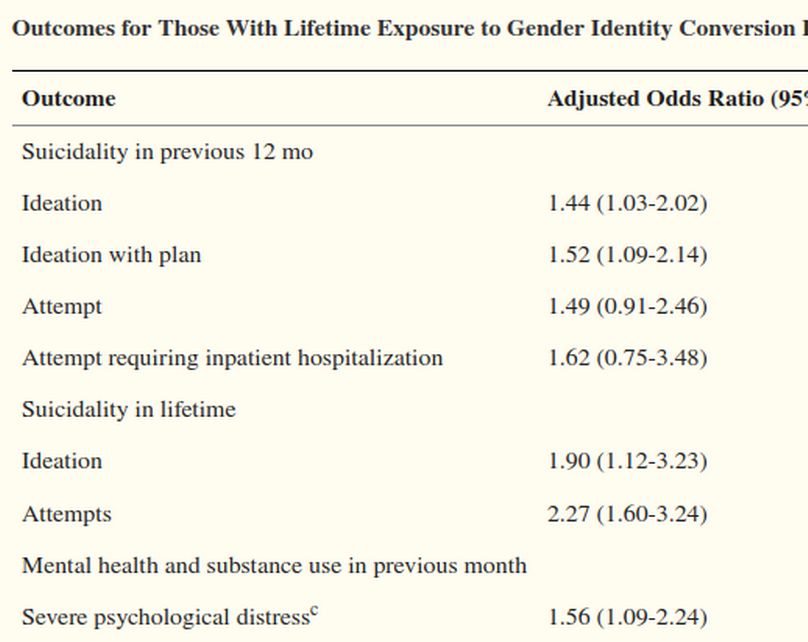
The third study using the same 2015 self report survey data set as the first two studies is a 2019 study called “Association Between Recalled Exposure to Gender Identity Conversion Efforts and Psychological Distress and Suicide Attempts Among Transgender Adults.” Here is a link to this study: https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2749479
The most important finding of this study was that there was no significant differences found when comparing exposure to Gender Counseling (GICE) by secular professionals vs religious counselors. Thus, the claim that religious counselors try to manipulate subjects with a Christian Guilt Trip is false. Instead, they likely try to understand the child in nearly the same way that a secular counselor does – by asking the child questions about their experiences and feelings related to those experiences.
There were some unexplained problems of this study. The first is that the average age in this study was about 9 years older than in the two previous studies (31 years versus about 22 years). 71% had spoken to a professional about their gender identity and only 20% claimed that there counselor had attempted to change their gender (which the study called Gender Identity Change Exposure or GICE). Participants were excluded from analyses if they did not report ever discussing their gender identity with a professional.
Outcomes were compared among respondents who reported exposure to GICE before the age of 10 with outcomes among those who endorsed lifetime exposure to therapy without GICE.
Overall, only 206 or one percent out of more than 20,000 respondents of reported discussing their gender identity with a professional also reported exposure to GICE before age 10 years. Only 17 out of the 206 where under the age of 25 as of 2015. This means that less than one tenth of one percent of transgenders reported being exposed to Gender Conversion after the year 2005. The most unusual finding was that 50% of those exposed to counseling before Age 10 suffered from a high level of “stress in the previous month” even though they had not been in counseling for more than 10 years.
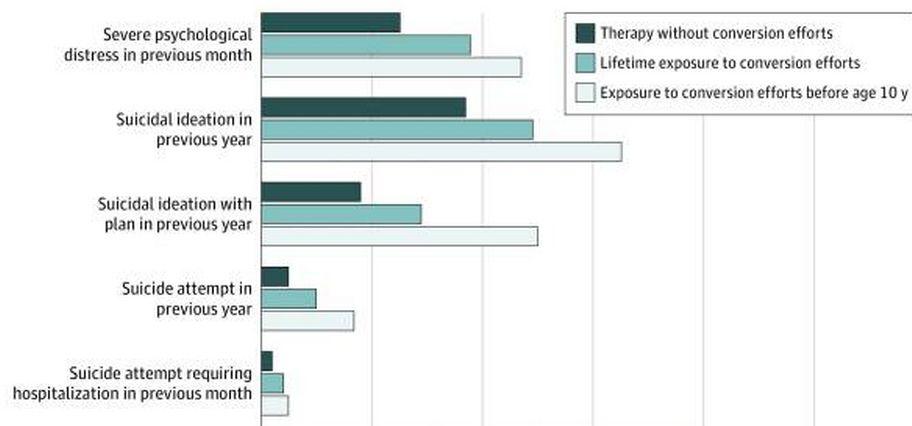
This indicates that this group is suffering from some serious mental health problems and likely has been suffering since their early childhood. In other words, the high level of Lifetime Suicide attempts is not due to the fact that they had counseling before Age 10, it is more likely to be due to the fact that they suffered four or more Adverse Childhood Events before they were five years old and before they ever had any counseling. What we can say is that this study does not prove that giving gender confused kids counseling before the age of 10 somehow caused them to commit suicide – or even caused them to be distressed 10 or more years later.
Fourth Study 2020 Adverse Childhood Experiences study
The next study is called “Sexual Orientation Change Efforts, Adverse Childhood Experiences, and Suicide Ideation and Attempt Among Sexual Minority Adults, 2016–2018.” Here is a link to this study: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7287530/
Experiencing SOCE was measured by this question: “Did you ever receive treatment from someone who tried to change your sexual orientation (such as try to make you straight/heterosexual)?”
Only 7% (n = 108) experienced SOCE from any source. Participants without SOCE had an average of 3.3 ACEs and those who experienced SOCE had more than 4.2 ACEs. Thus, it is almost certain that those subjects taken to counselors had much more serious mental health problems due to adverse events occuring before age 5 which then led to counseling later in childhood. So once again, we are talking about two completely different groups of subjects.
Compared with not experiencing SOCE, experiencing SOCE was associated with twice the odds of lifetime suicidal ideation, 75% increased odds of planning to attempt suicide, 88% increased odds of attempting suicide resulting in no or minor injury, and 67% increased odds of suicide attempt resulting in moderate or severe injury.
The most accurate event of the self reports was Attempted Suicide, moderate to severe injury – as this indicates an event which might be documented. 12.8 % of those with no SOCE attempted suicide and 15.7% of those who did have SOCE attempted suicide. This is much lower than the 2015 self reports which concluded that about 50% of transgenders had a lifetime suicide attempt.
The only way to explain this huge difference is that the vast majority of subjects in this study were not actually transgender. It is important to avoid mixing apples with oranges. Our concern is giving drugs to gender confused children who claim to be Transgender. This at risk Transgender group should not be lumped together with LGB youth who are not interested in taking Trans drugs or changing their biological sex.
In addition, we do not know the average age of the subjects in each group. As noted from the previous studies, it is likely that those experiencing SOCE are much older and therefore have a longer period of time to accumulate lifetime suicide events.
Finally, this study did not report whether suicide attempts happened before or after SOCE. Thankfully, a followup study did research this question and found that the suicide attempts happened BEFORE SOCE. We review this followup study later in our report. But this is a perfect example of how false conclusions are arrived at when the wrong questions are asked.
Studies refuting the claims made by Bob Ferguson
This ends the studies provided by Bob Ferguson. None of them actually concluded what Ferguson claimed they concluded. We wll next look at a series of studies confirming that counseling helps gender confused children while giving them toxic drugs harms them.
2022 Reanalysis of "Sexual Orientation Change Efforts, Adverse Childhood Experiences, and Suicide Ideation and Attempt Among Sexual Minority Adults, 2016–2018
Recall that in our last study, we pointed out that those with 3 Adverse Childhood Events are likely to be a different group than those with 4 adverse childhood events and we pointed out that it is important to know whether suicide attempts occurred before or after SOCE as sucide attempts occuring before SOCE can not possibly be caused by SOCE!
The 2022 Reanalysis is called “Do Sexual Orientation Change Efforts SOCE increase the suicide risk for sexual minorities?” You can download this 75 page study from this link:
https://first-heritage-foundation.s3.amazonaws.com/live_files/2024/01/Sullins-2022-vs-Blosnich-2020-Do-sexual-orientation-change-efforts-SOCE-increase-suicidal-risk-for-sexual-minorities-an-exchange.pdf
Paul Sullins, a senior research associate at The Ruth Institute, and former sociology professor at Catholic University, found that SOCE actually sharply decreased the risk of suicide or thoughts of suicide.
"What we're left with is a situation where we're being fed a lie that somehow attempting to change sexual orientation is going to fail all the time and it's going to cause harm, and the truth is just the opposite," Sullins told "The Daily Signal Podcast."
Sullins analyzed the data from a study conducted in 2020 by John Blosnich. The study, "Sexual Orientation Change Efforts, Adverse Childhood Experiences, and Suicide Ideation and Attempt Among Sexual Minority Adults, 2016–2018," used data collected by the Gallup Organization. Gallup called over 330,000 Americans to screen about 3,000 who identified as LGB and then collected 1,500 interviews on the issue.
With that data, they correlated the amount of suicide ideation and other suicidal behaviors, such as making a plan to commit suicide or suicide attempts. They correlated those with whether a person had ever been to SOCE and found that subjects who had been to SOCI had over twice the rate of suicidal thoughts and were 1 .7 times as likely to attempt suicide. On the basis of this, calls for banning SOCE were moved forward. Yet Blosnich made an elementary mistake in analyzing the data. He had ignored one very crucial question, which was, 'When did you think about suicide?”
When Sullins read the interviews, he looked to see "whether the suicide activity happened before or after the person went to SOCE. What he found was that most of the suicidal behavior happened before the person ever went to SOCE. Two-thirds of the thoughts of suicide happened before they ever went to SOCE. So he published a rebuttal to the Blosnich study finding not only that SOCE did not increase suicidal behavior, it decreased it. Sullins results show that of the 89 SOCE participants who reported ever having thoughts of suicide, 58 (65%) of them did so before they underwent SOCE. Likewise, almost half of reported suicide planning (49%) and suicide attempts (48%) occurred before SOCE. When only suicidality during or after SOCE is considered, providing SOCE gender counseling on average reduced the suicide risk by 42%.
This is Table 1 which is on Page 75 of the Sullins analysis:
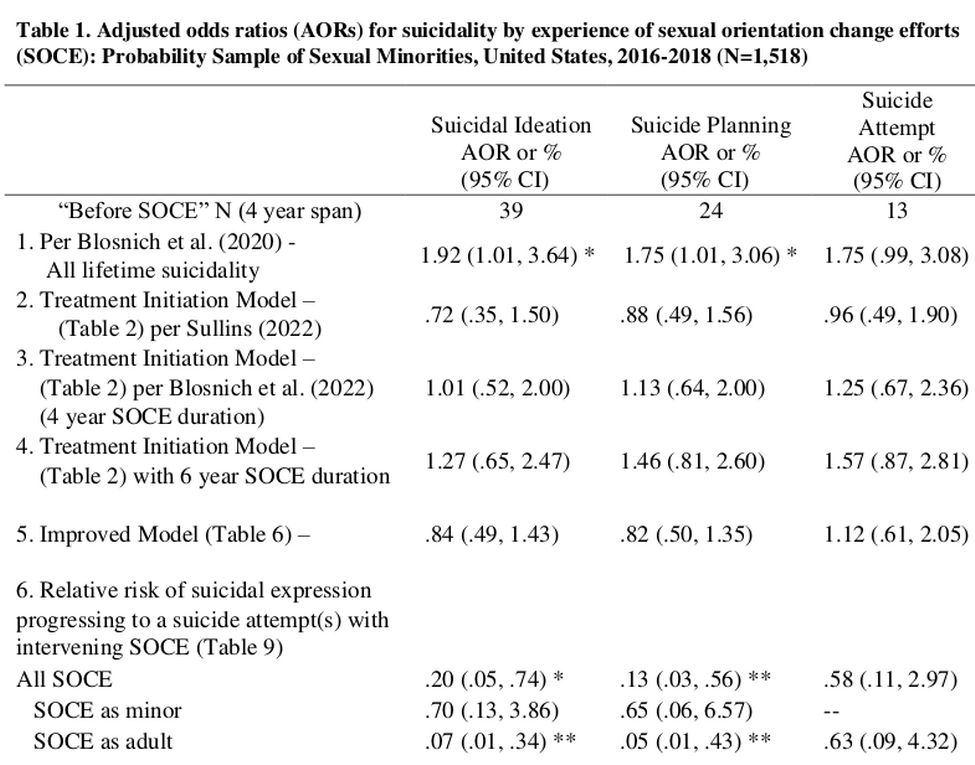
All of the odds ratios above are in comparison to the No SOCE odds being 1.00. Therefore, odds of 1.20 would be an increased risk of 20% while odds of 0.80 would be a reduced risk of 20%. Row 1 is the misleading result, as it ignores for time-order of only including attempted suicides that occurred during or after counseling, and thus falsely claims that gender counseling (SOCE) increases the odds of a suicide attempt by 75%.
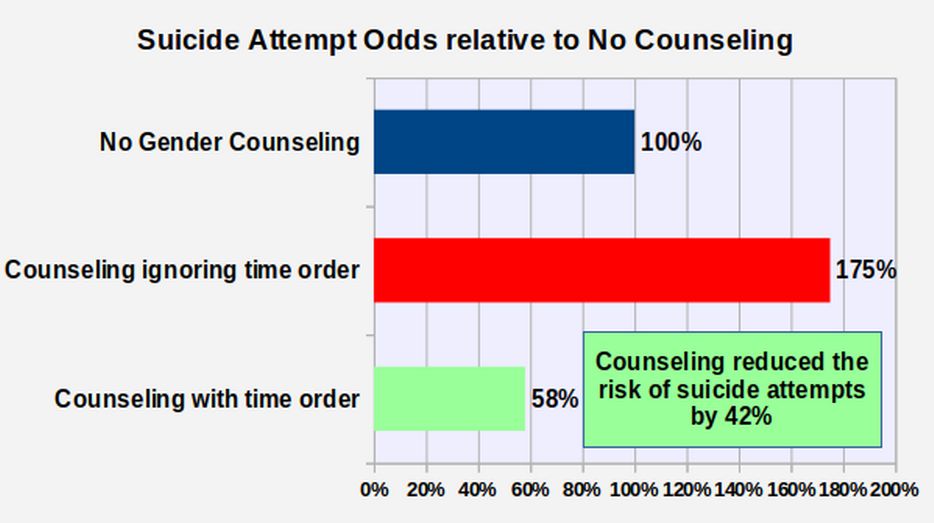
The most important row is the third row from the bottom which shows that giving gender counseling on average reduced their suicide risk by 42%. Here is a table of this difference:
|
Counseling Options |
Odds relative to No SOCE |
|
No Gender Counseling (No SOCE) |
1 |
|
Gender Counseling ignoring time order |
1.75 |
|
Gender Counseling including time order |
0.58 |
Here is a graph of this difference based on the above table:
Why accounting for the Time Order of Events Matters
Failing to account for the time order of events will often lead to a conclusion that is the exact opposite of the actual effect of any intervention. For example, it is well known that taking small daily amounts of aspirin can reduce the risk of a heart attack. Therefore, those who have already had a heart attack often take a small amount of aspirin every day to reduce their chances of having a future heart attack. But imagine that a careless researcher studied these heart attack prone people. The careless researcher would certainly find a relationship between taking aspirin and “lifetime occurances of heart attacks.” Now imagine that based on this relationship, the careless researcher ignored the time ordering of events. This would cause this researcher to falsely claim that taking aspirin caused the heart attacks and therefore that taking aspirin should be banned! This turns out to be the flawed logic behind nearly every study claiming that SOCE causes suicides and should be banned.
In 2022, C. H. Rosik published a review called “A wake-up call for the field of sexual orientation change efforts research”. Here is a link to his review: https://doi.org/10.1007/s10508-022-02481-7
In his review, Rosik provides the following Table of 20 Anti -SOCE studies – every one of which failed to account for the time order of events by including suicide attempts that occurred before any SOCE was provided:
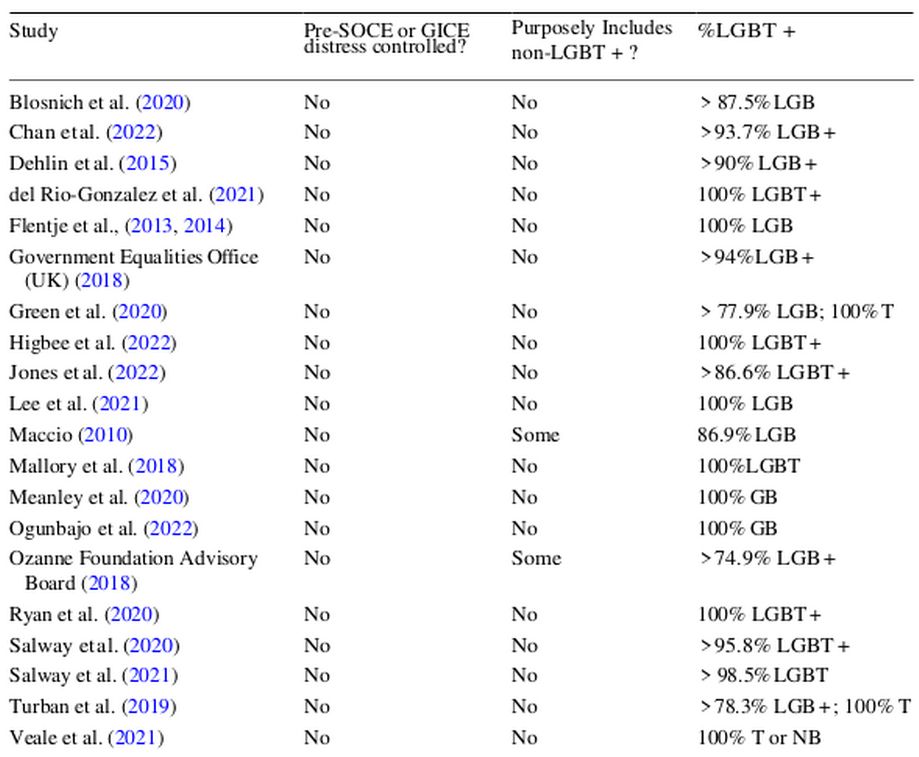
In short, Anti-SOCE research is based on a House of Cards that fell over thanks to the re-analysis provided by Sullins. We will next review two recent studies both of which confirmed the benefit of gender counseling.
2021 Efficacy and risk of sexual orientation change efforts (SOCE)
This next study, called “Efficacy and risk of sexual orientation change efforts: a retrospective analysis of 125 exposed men” takes a much closer look at the actual effects of SOCE compared to the 2015 Self Report Surveys. Here is a link to this study: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8080940/
This study surveyed 125 men who had completed or were in the process of SOCE. At the time of the survey, 42% were still pursuing SOCE and 58% had concluded SOCE. Median time post-SOCE was about 3 years. Participants reported seeking various kinds of help for their conflicted sexuality. The most frequently were religious support groups (81%), pastoral counselors (70%), marriage or family counselors (61.3%), psychologists (57%), non-religious support groups (52%), psychiatrists (26%) and social workers (21.8%).
For all three components of sexual orientation—attraction, identification and behavior—average same-sex orientation in the sample significantly declined following SOCE intervention.
Prior to SOCE participation, the large majority of married men (71%) engaged in homosexual sex. After SOCE, that proportion plummeted to only 14%, and was only about half as prevalent among the married men as among unmarried men. From the standpoint of the men in the sample, one of the most important indications of perceived SOCE efficacy may be its association with drastically reduced unwanted same-sex activity which conflicts with the religious norms of their marriages.
Exposure to SOCE was associated with significant declines in same-sex attraction and sexual activity (2.4 to 1.5 on a 4-point scale of frequency). From 45% to 69% of SOCE participants achieved at least partial remission of unwanted same-sex sexuality; full remission was achieved by 14% for sexual attraction and identification, and 26% for sexual behavior.
SOCE related to six psychosocial areas: self-esteem, social functioning, depression, self-harm, suicidality, and alcohol or substance abuse. For all six areas the participants experienced both positive and negative changes, however the positive changes were stronger and more widely distributed than the negative changes. The positive changes affected from 17% (for alcohol abuse) to 94% (for self-esteem) of participants, whereas the negative changes were reported by only 5% (for alcohol abuse) to 33% (for depression) of participants. The experience of marked or extreme positive changes ranged from 12% to 61%, while equally strong negative changes only ranged from 1% to 5%. For all six areas the net change, which is the summative index of both positive and negative changes, was a positive number greater than zero. This indicates that, considering both positive and negative changes, the net effect of SOCE for each area was positive. The strongest net positive effect was for depression. Almost three-fourths (73.2%) of respondents reported positive changes in depression due to SOCE, while two-thirds (66.1%) reported no negative changes in depression. Only 2.4% (3) of (125) participants experienced marked or extreme negative changes in suicidal thoughts or attempts as a result of SOCE, while nine times that number (28) (21.8%) experienced similarly strong positive changes in suicidality. 75% were about the same.
2017 Stephen H. Black, The Complete First Stone Ministries Effectiveness Survey Report
https://www.csmedia1.com/firststone.org/the-complete-fsm-effectiveness-survey-report-pdf.pdf
The second pro-SOCE study is from First Stone Ministries - a Christian ministry based in Oklahoma City that focuses on “overcoming all forms of sexual brokenness including homosexuality, sexual abuse and addiction to pornography.” They took a survey of clients who had participated in their ministry’s programs over a 25-year period (1990-2015). In the end, 185 former clients completed the First Stone survey.
This survey provides detailed information on the experiences of many people who have undergone Christian-based counseling. Of those who came to the ministry with same-sex attractions (67 percent of all clients), 23 percent reported an elimination of all same-sex attractions. Questions focused more on behaviors showed dramatic results— 78 percent said that the ministry had helped them “in overcoming [some] form of sexual sin and/or brokenness.” And of those who reported that they had a “sexual addiction” before coming to First Stone (61 percent of the total), an amazing 93 percent no longer considered themselves “addicted” at the time of the survey. As for harm, of 98 respondents who wrote concluding comments, 85 were positive, only 7 were negative, and 6 were mixed.
A certain percentage of the LGBT-identifying population will have negative experiences whether they have undergone SOCE or not. To scientifically prove that SOCE is generally “harmful,” one would have to prove that all of the following are true:
- The number of clients who report harm from SOCE exceeds those who report benefits;
- Negative mental and physical health indicators among those who have undergone SOCE exceed those among persons who have undergone alternative “gay-affirming” therapy;
- Negative mental and physical health indicators among those who have undergone SOCE exceed those among persons with same-sex attractions who have had no therapy at all.
- Negative mental and physical health indicators among those who have undergone SOCE exceed those among persons who have had therapy or counseling for other conditions.
There simply is no scientific evidence to prove each of these points. If critics of SOCE claim there is “no evidence” that it can ever be effective in changing any client’s sexual orientation, they are simply wrong.
US Study finds giving kids toxic drugs increases their risk of suicide
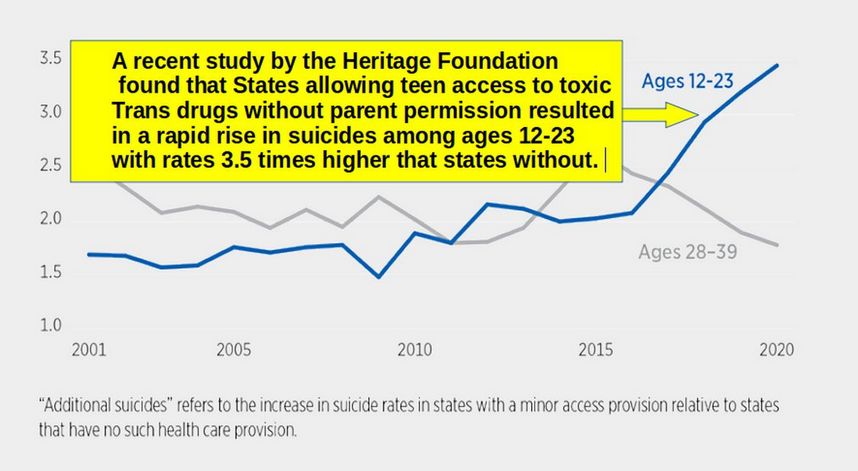
Here is another study confirming that giving kids trans drugs does not reduce their risk of suicide. States that started giving kids Trans Drugs in the past 9 years have seen a dramatic rise in the number of suicides between the ages of 12 to 23 to the point that the rate is now 3 and a half times higher than in states where kids are not given trans drugs.
https://www.heritage.org/gender/report/puberty-blockers-cross-sex-hormones-and-youth-suicide
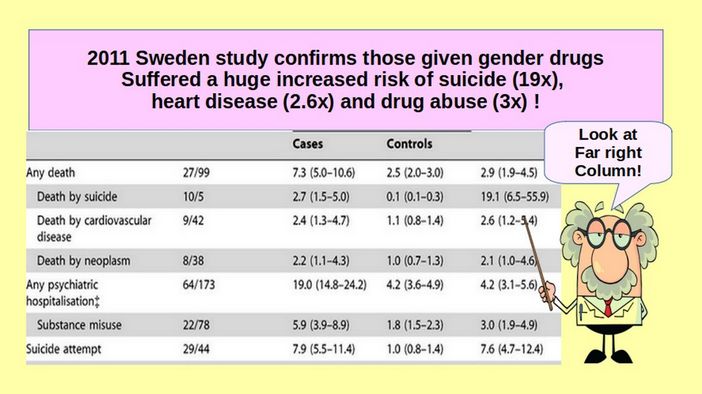
A study of transgender patients from Sweden found 30 years after surgery, the rate of suicide among post-operative transgender adults was nearly 20 times greater than that of the general population. See Cecilia Dhejne, et al., Long-term Follow-up of Transsexual Persons Undergoing Sex Reassignment Surgery: Cohort Study in Sweden, (Feb. 22, 2011) https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0016885
Look at the far right column in this table to see the risk ratio for transgender adults compared to control adults. For example, those who had gender mutilation surgery were 3 times more likely to abuse drugs.
While giving kids toxic drugs increases the suicide rate, giving them counseling reduces the suicide rate.
There are now several studies confirming that drugs do not solve mental health problems and that counseling is a much better option to reduce the risk of suicide. For example, a 9 year study in Australia found that giving minors gender mutilation drugs did not improve their mental health. Before taking the drugs, 88.6% suffered from mental health problems. After taking the drugs, in a follow up 9 years later, 88% still suffered from their mental health problems. https://www.mdpi.com/2227-9067/10/2/314
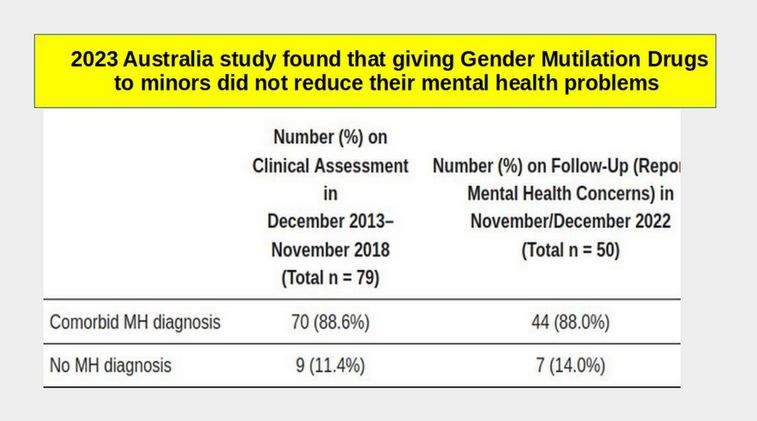
This study, an others like it is why nations from around the world including Sweden, Norway, the UK, Denmark, Finland, France and Australia, have all moved away from giving gender confused kids toxic gender drugs and instead now recommend that these kids be provided with counseling to address their underlying mental health problems.
Studies on the benefits of counseling to reduce suicidal thoughts
A 2019 review of 40 studies on counseling found that 37 (92%) concluded that counseling reduces both suicidal thoughts and suicide attempts. https://www.frontiersin.org/journals/psychology/articles/10.3389/fpsyg.2019.00277/full
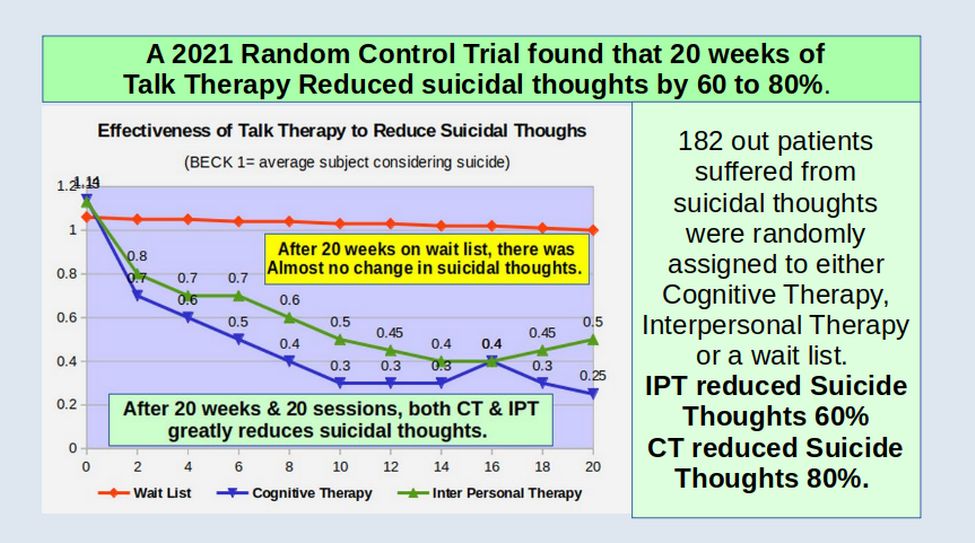
2021 Study finds Talk Therapy greatly reduces Suicidal Thoughts
The two most common psychological treatments for depression and suicidal thoughts are cognitive therapy (CT) and interpersonal therapy (IPT). Cognitive Therapy relies on changing a persons thoughts in order to improve their feelings. Inter Personal Therapy helps a person deal with their feelings about past negative events. Most child counselors use a combination of both. In 2021, van Bentum et al. Published a study called, “Cognitive therapy and interpersonal psychotherapy reduce suicidal ideation” Here is a link to this study.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8451935/
Here is their description of their study: “We tested whether CT and IPT outperformed the wait‐list control group by comparing change in Beck Depression Inventory suicide item scores. A total of 182 outpatients, aged 18–65 years, were included and randomly assigned to one of three conditions: CT (n = 76), IPT (n = 75), or a Wait List followed by treatment of choice (n = 31). Each intervention consisted of 20 weekly sessions of 45 min. Treatments were performed by 10 licensed psychologists, psychotherapists, and psychiatrists (five in each condition) with an average 9.1 years of experience.”
The result was that the Wait List subjects had almost no change while the IPT group had a 60% reduction in Suicidal thoughts and the CT group had an 80% reduction.
This combination of studies showing that drugs do not work while counseling does work led Sweden to move away from recommending gender mutilation drugs and towards counseling as the best option for minors. Sweden concluded the risks of puberty blockers and sex hormones outweigh any benefits. They stated that “Health care should not provide interventions that we do not know to be safe and beneficial.”
2023 Psychosocial Functioning in Transgender Youth after 2 Years of Gender Hormones
One of the main claims made by those who advocate giving drugs to gender confused kids is that giving them drugs will reduce their suicide rate. The claim has never been supported by any actual scientific evidence. But it has been repeated thousands of times. Recently a study was published which analyzed the mental health of 315 trangender kids from 2020 to 2022 who were given cross sex hormones at the Seattle Childrens Hospital Gender Clinic. One of the adverse side effects was listed as “two fatalities.” Here is a link to their study. https://www.nejm.org/doi/full/10.1056/NEJMoa2206297
Remarkably, the clinic had the audacity to issue a press release claiming that giving these kids drugs helped improve their mental health. But here are the facts. One suicide per 315 kids is a rate of 317 suicides per 100,000 kids. Two suicides was a rate of 634 suicides per 100,000 kids. The national rate for kids age 12 to 20 is 14 per 100,000. So a rate of 634 suicides per 100,000 is 45 times the national average suicide rate for this age group. This is even higher than a Sweden 2011 study that found the suicide rate of Transgender subjects giving both drugs and surgery was 19 times higher than the general population.
Equally concerning, this study took in a huge amount of data on the suicidal thoughts of subjects during this two year study and then at the last minute decided not to publish this data. Why? The only possible reason is that this data confirmed what we already know – that giving kids transgender drugs does not reduce their suicide rate. What these kids need is counseling – which is now banned in 23 states – including Washington.
If Seattle Childrens Hospital was actually interested in learning the truth about giving kids drugs, here is what they would really do. Take the next 300 Transgender kids and randomly assign them to either a all-drugs no counseling group or an all-counseling, no drugs group. If parents wanted, there could also be an all-drugs, all-counseling group. Then study them not just for 2 years, but for 10 years. Wait. This Random Control Trial is not currently possible in Washington state because we have a law that prohibits giving kids just counseling and no drugs. So before we can do this study, we first need to repeal the crazy All Drugs and No Counseling law. So the first step in learning the truth is replacing our crazy legislators.
The Chilling Effect of Gender Conversion Bans on Child Counseling
My own background in child counseling goes back to 1972 when I had the honor of taking a course on child counseling from Carl Rogers, the author of Freedom to Learn. I wrote my Senior paper on combining his child development theories with those of Abraham Maslow, author of Toward a Pyschology of Being and creator of Maslow’s Hierarchy of Human Needs. Since then, as a teacher and child development researcher, I have been honored to know many child counselors during the past 52 years. None of these child counselors have ever used or advocated for any threatening, shaming or coersive techniques. At the same time, I doubt that few if any traditional child counselors would support the idea of giving a giving a gender confused child experimental toxic drugs rather than helping the child deal with their underlying mental health problems which are well known to be the result of adverse childhood events.
Thus the term Conversion Therapy appears to be a Red Herring invented by those promoting giving children so-called Gender Affirming Drugs. State laws banning “Gender Conversion” are really laws promoting toxic gender drugs. Conversion therapy is then broadly defined to mean anything that fails to support affirming the made up beliefs of a gender confused child and anything that discourages the use of toxic gender drugs. State laws banning Conversion Therapy have the effect of enshrining gender drugs as the sole acceptable approach to assisting transgender youths – because what these laws really do is ban not just the Red Herring of Conversion Therapy – but also traditional child counseling.
Rather than risk being turned into the state, taken to court, fined thousands of dollars and/or losing their license, many traditional child counselors either refuse to work with gender troubled children. Many others have been forced into an early retirement.
Parents rightly fear that taking their child to an explicitly gender affirming therapist will lock their child into the deadly path of the Transgender Cult and gender drug addicition. But as a result of these State bans on traditional child counseling, many parents find it difficult to find a child counselors willing to take any stance other than that of state-approved, drug-promoting “gender-affirmation.”
Worst of all, gender confused children, nearly all of whom suffer from serious mental health problems, fail to get the counseling they urgently need. Instead, all at-risk children are offered is ineffective toxic drugs and lies about how they can change their gender into the other gender simply by changing their name and pronouns. As the British High Court recently ruled, it is impossible for any young child to understand the long term negative consequences of being sterile for life and being addicted to toxic drugs for life.
How to Create a Better Future for all Children
As a result of Ferguson’s new rules, tens of thousands of children in our state have been misled into a horrible life of taking a never-ending stream of toxic drugs to “affirm” Ferguson’s other Big Lie – that it is possible for a child to change their gender from a boy to a girl or a girl to a boy merely by changing their pronouns as if changing ones pronouns and pretending to be a different sex will somehow will solve one’s underlying mental health problems. Once again, the Truth eventually comes out.
There are three steps to solving this Transgender Takeover of our schools and our kids.
The first step is Education. Parents and Grandparents need to take the time to get better informed about the drawbacks of the Transgender Cult and the danger it presents to their children and to all children. The scientific research is out their and more studies are being published every week on the drawbacks of drugging children.
The second step is Political Organization. Parents need to reach out to other parents in their community and become more involved in the election process. Corrupt politicials often receive huge amounts of funding from the drug companies that benefit from laws that promote getting kids addicted to their toxic drugs. Corrupt politicials also get millions of dollars in free advertising from the mainstream media which in turn is funded by millions of dollars in drug company ad money. The only way for an honest candidate to compete against the drug pushers and their accomplices is with the support of parents willing to take the time to get politically involved and help their campaigns with either time, money or both.
The third step is taking legal actions to oppose laws that restrict the rights of child counselors. Both parents and counselors need to have the courage to go to court to defend the rights of parents and counselors to freedom of speech and to defend the rights of children to hear diverse points of view and have access to a wide range of counseling options. Legal actions to restore parents rights are the topic of our next article.
What’s Next?
This completes our article on why gender confused children are harmed by toxic transgender drugs and why what they really need is gender counseling to address their underlying mental health problems. In the next article, we will summarize the legal history of why banning gender counseling violates all of our rights under the First Amendment.