This report is divided into an Introduction followed by 25 sections. Click on ALL PAGES at the bottom of this Table of Contents to read the entire article on one web page. Click on the Introduction link or click Next to read just the Introduction. You can then click on any of the section links in the Table of Contents to read any section of the report you are interested in learning more about.
Introduction… Why We Must Stop the Gender Mutilation Racket
In this report, we provide scientific evidence that promoting gender mutilation of minors is state-sponsored child abuse. We should begin by noting that this report is not an attack on Transgender people or an attempt to control how people choose to live their lives after they become adults. Instead, this is a report on why specific, cancer-causing drugs, including puberty blockers and cross-sex hormones, should not be given to children under the age of 18. This report is focused solely on the right of children to be raised in a drug-free environment where they will have the greatest chance of having a happy childhood and growing into happy, productive adults.
The drug industry uses the term “Gender Affirming Care” to describe giving children these toxic drugs. We maintain that this term misleading both to parents of gender-confused children and to the public. We will therefore use the term “Gender Mutilation” to describe giving these toxic drugs to minors – as the end result of giving minors these experimental drugs is that their sex organs will be mutilated and the child will become sterile.
In addition, puberty blockers have been known to cause brain tumors. In July 2022, the Food and Drug Administration (FDA) in the US issued a warning label about the risk of puberty blockers after six minors (ages 5-12) experienced severe symptoms of tumor-like masses in the brain.
In addition, in this report, we provide several studies linking cross sex hormones to huge increases in cancer rates.
You will see throughout this report that real child development experts recommend child and family counseling as the best option for resolving problems. The goal is to help the child learn coping skills and other problem solving skills to resolve their issues.
Child Development should be based on Science not Politics
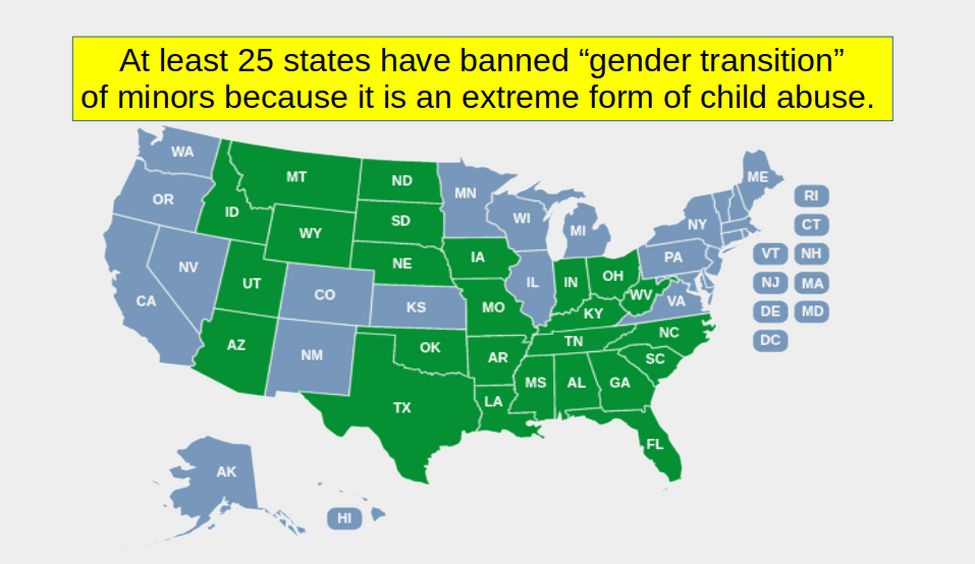
We recognize that in recent years, this subject has become a political football in the United States. Currently, about 25 states led by Republicans have passed laws banning gender mutilation of minors.
Meanwhile 20 State Attorney Generals of states led by Democrats have filed legal briefs in favor of gender mutilation of minors. Sadly, these State Attorney Generals promoting gender mutilation of minors include Washington Attorney General Bob Ferguson who is current running for Governor of Washington state. Voters in Washington state need to know that if Ferguson is elected Governor this year, the future of hundreds of thousands of children in our state will be put at risk.
We will look at a couple of misleading claims made by Ferguson in his legal brief in a moment. First, we will look at the recent changes to policies on banning gender mutilation of minors in Europe, where science rather than politics seems to be better recognized. Here is a brief summary of recent changes by country.
Sweden: While Sweden was the first country in the world to allow people to legally change their gender in 1972, it has recently moved away from recommending gender mutilation drugs and towards counseling as the besst option for minors. In 2022, the Swedish government’s National Board of Health and Welfare published a study concluding that puberty blockers and hormone treatments for minors “should be provided only in exceptional cases,” adding that the risks of puberty suppressing drugs and gender-affirming hormones currently outweigh the possible benefits. “Health care should not provide interventions that we do not know to be safe and beneficial,” Mikael Landén, a professor and chief physician at the University of Gothenburg in Sweden and co-author of the report. https://pubmed.ncbi.nlm.nih.gov/37069492/\
United Kingdom: Children at schools in the United Kingdom will no longer be taught gender identity after a several hundred page study called the Cass Review was published in February 2022 finding that the curriculum was extremely harmful to child development. The study of gender identity services for children and young people was written by Dr Hilary Cass, past president of the Royal College of Pediatrics and Child Health.

Denmark: In 2023, a major medical journal Ugeskrift for Læger, the Journal of the Danish Medical Association, confirmed that there has been a marked shift in the country’s approach to caring for youth with gender dysphoria. Most youth referred to the centralized gender clinic no longer get a prescription for puberty blockers, hormones or surgery. Instead they receive therapeutic counseling and support. https://segm.org/Denmark-sharply-restricts-youth-gender-transitions
Finland: After years of research, in 2020, a public health body in Finland concluded that “medical gender reassignment is not enough to improve functioning and relieve psychiatric comorbidities among adolescents with gender dysphoria.” They therefore now recommend that minors experiencing gender dysphoria first be provided with counseling and, if further medical treatment is pursued, that the patient be made “aware of the risks associated with these drugs.” https://pubmed.ncbi.nlm.nih.gov/31762394/
France: In February 2022, the French National Academy of Medicine recommended the “greatest reserve” when considering puberty blockers or hormone treatments due to possible side effects such as “impact on growth, bone weakening, risk of infertility.”

Norway: In 2023, the Norwegian Healthcare Investigation Board concluded that “Gender Affirming Care is not evidence based” and thus recommended that gender-affirming care drugs such as puberty blockers be defined as experimental.

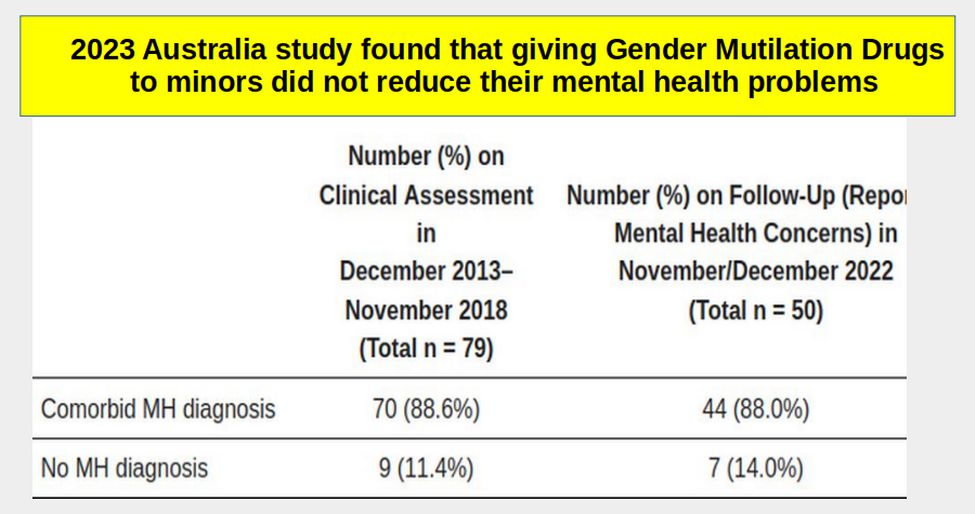
Australia: A 2023 long term 9 year study in Australia found that giving minors gender mutilation drugs did not improve their mental health. Before taking the drugs, 88.6% suffered from mental health problems. After taking the drugs, in a follow up 9 years later, 88% still suffered from mental health problems. https://www.mdpi.com/2227-9067/10/2/314
The shifts in policy in these nations and the research underlying these shifts were summarized in a report published in 2023. Here is the link: https://link.springer.com/article/10.1007/s11930-023-00358-x
Here are some quotes from this report: “Results of long-term studies of transgender populations failed to demonstrate improvements in mental health, and suggest there are treatment-associated harms. Public health authorities in Finland, Sweden, and England concluded that the risk/benefit ratio of youth gender transition ranges from unknown to unfavorable. As a result, there has been a shift from “gender-affirmative care,” to a more conservative approach that addresses psychiatric comorbidities.”
“Evidence does not support the notion that “affirmative care” of today’s adolescents is net beneficial. Despite claims of the lifesaving nature of gender transition for adults, none of the many studies convincingly demonstrated enduring psychological benefits. The longest-term studies, with the strongest methodologies, reported markedly increased morbidity and mortality and a persistently high risk of post-transition suicide among transitioned adults.”
Blatant lies made by Washington Attorney General Bob Ferguson in his legal brief

In August 2022, Bob Ferguson along with 19 other Attorney Generals from Democrat led states, filed a legal brief in a federal case challenging an Alabama law which banned giving gender mutilation drugs to minors. Here is a link to the brief: https://www.splcenter.org/sites/default/files/documents/eknes-tucker-v-marshall-states-amicus.pdf
The judges for the Court of Appeals ruled against Ferguson and in favor of Alabama concluding that Alabama had a right to regulate drugs with known risks being given to minors and that the Alabama law did not discriminate against Transgender people because the law applied to all children. This case and several others will be reviewed by the US Supreme Court in October 2024. Given the mountain of science on the drawbacks of giving gender drugs to minors, it is likely that the US Supreme Court will also rule against Ferguson and in favor of the 25 states that have banned giving gender mutilation drugs to minors.
Later in this report, we will review several more studies on the drawbacks of giving gender mutilation drugs on minors. Here, as examples of how badly misinformed Ferguson is on consequences of gender mutilation of minors. we will look at two studies cited by Ferguson that he claimed were in favor of giving kids gender mutilation drugs Here is an example of an extremely misleading quote from the Ferguson legal brief:
“A survey of over 3,500 transgender adults found that individuals who received pubertal suppression during adolescence had almost 20 percent lower odds of lifetime suicidal thoughts compared to individuals who wanted this treatment but did not receive it.”
This quote was one of several in the Ferguson brief claiming that those given gender mutilation drugs had better outcomes than those who were not given gender mutilation drugs. However, the actual study had a radically different conclusion. Here is a link to the study this claim was based on: https://publications.aap.org/pediatrics/article/145/2/e20191725/68259/Pubertal-Suppression-for-Transgender-Youth-and
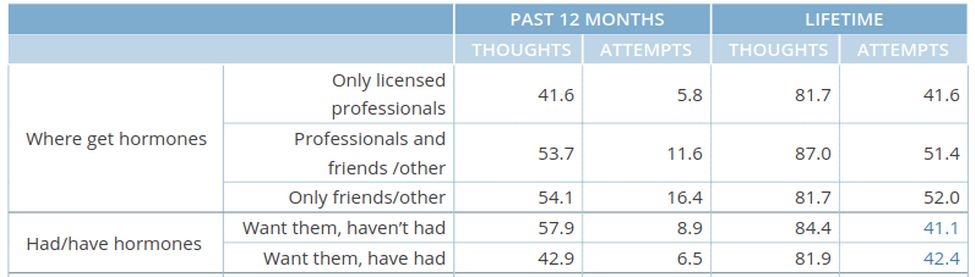
Here is the actual table of outcomes in the study:
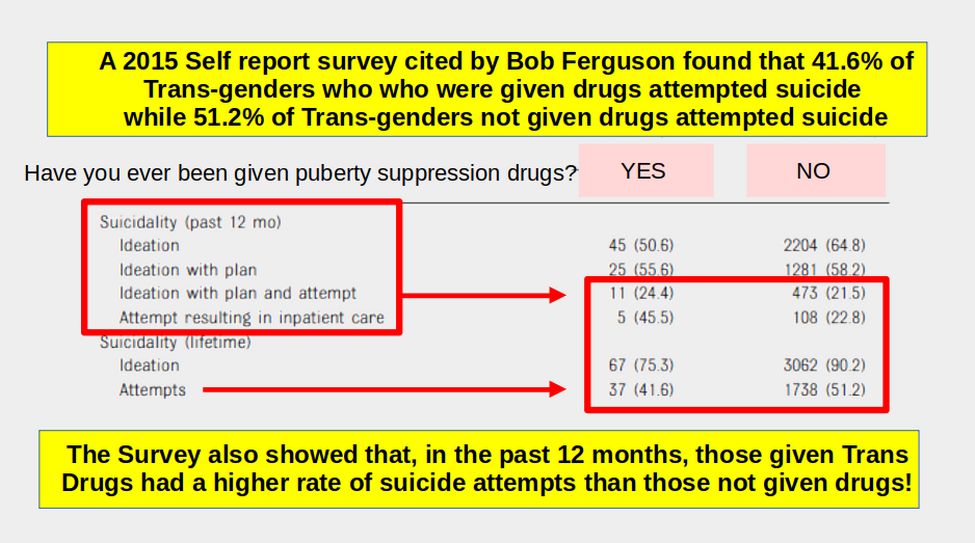
The study found that 90.2 percent of those not given drugs thought about committing suicide while 75.3 percent of those given drugs thought of committing suicide. The difference is 15% - not 20% claimed by Ferguson.
But much more important, 45.5% of those given gender mutilation drugs attempted to commit suicide in the previous 12 months with the attempt putting them in the hospital. Meanwhile, only 22.8% of those not given gender mutilation drugs had a suicide attempt that put them in the hospital.
To understand how both of these “facts” can be true, all we need to do is look at the average age of those given drugs versus those not given drugs. Here is Table 1 showing the claimed age difference:
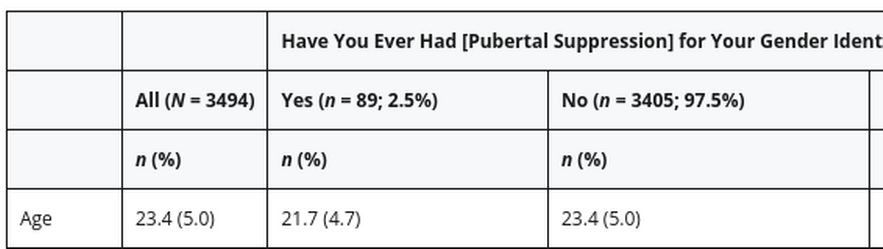
Note that the average age for the entire sample was 23.4 which was also the average age for those not given drugs. Meanwhile, the average age for those given drugs was only 21.7. But a huge flaw of this online self report survey was that the minimum age to take the survey was 18. Also, the most common response for age was 18 – which clearly indicates a non-random response. In fact, it is certain that many 16 and 17 year olds took the survey and checked the 18 box because there was no 16 ot 17 box. These younger people were very likely to be in the group given drugs since government payment for those drugs in the US was only available since passage of the Affordable Care Act 4 years before the survey. When we adjust for this fact, the actual age of those given Trans drugs is about 20.
In addition, it is known that suicide risk is much higher, Trans or Not, after the onset of puberty. We will assume puberty starts at age 12. Thus the Trans Drug group had a Suicide “Lifetime” of 20 minus 12 equals 8 years while the Trans No Drug group had a Suicide “Lifetime” of 23.4 minus 12 equals 11.4 years. Therefore, the Trans Drug group Suicide Attempts Percent per year was 41.6% divided by 8 years equals 5.2% percent per year. Trans No Drug group Suicide Attempts Percent per year was 51.2% divided by 11.4 years equals 4.5% per year. Combining this fact with the fact that in the previous 12 months before the survey, the Trans Drug group had more suicide attempts than the Trans No Drug group, it becomes obvious that giving drugs to transgender youth increases their rate of suicide – for the equally obvious reason that Trans drugs do not deal with the underlying mental health problems like Depression that led to the Gender Confusion in the first place. In short, the data from this study leads to the opposite of the claim made by Bob Ferguson and his accomplices.
What caring, rational person would advocate spending hundreds of millions of dollars giving tens of thousands of minors gender mutilation drugs when the result of giving them those drugs results in a huge increase in suicide attempts that result in hospitalization?
As you may know, no one is allowed to blatantly lie to a court. It is called perjury. But an attorney has a special duty to not lie to a court. And an Attorney General needs to be held to an even higher standard. But here, Ferguson did not just lie to any county or state court or even any federal court. He blatantly lied to the federal Court of Appeals which is only one step below the US Supreme Court.
But he did not merely lie to the Court of Appeals, he lied to the American people, including millions of parents and children, about a gender mutilation policy that is currently harming millions of children and costing the tax payers billions of dollars.
In short, this may be one of the worst crimes Bob Ferguson has ever committed. The voters need to know about this crime because Ferguson is now running for Governor here in Washington state.
Here is another misleading claim made by Ferguson in his legal brief:
“A 2020 study found that adolescents who begin gender-affirming treatment at later stages of puberty were over five times more likely to have been diagnosed with depression and over four times more likely to have anxiety disorders than adolescents who seek treatment in early puberty.”
Ferguson claimed that this is why gender mutilation drugs need to be given to younger teenagers rather than waiting until they are age 18 adults and can therefore legally give informed consent. Once again, the actual study he cited to support this claim had a completely different explanation.
Here is a link to the actual study: https://publications.aap.org/pediatrics/article/146/4/e20193600/79683/Mental-Health-and-Timing-of-Gender-Affirming-Care
The study defined “early puberty” as 14 and “later puberty” as 16.
So Ferguson is claiming that kids who start gender mutilation drugs at 16 “were over five times more likely to have been diagnosed with depression and over four times more likely to have anxiety disorders” than kids who start gender mutilation drugs at 14.
Here is what the study actually found:
“78% of all youth reported one or more mental health problems. Depressive and anxiety disorders were reported by 40.0% of younger youths (average age 14) and 44.3% of older youth (average age 16). “
More Older Youths than Younger Youths reported depression (46% vs 30%), had self-harmed (40% vs 28%), had considered suicide (52% vs 40%), had attempted suicide (17% vs 9%).
Below is a chart of the differences between the two age groups (younger group in green and older group in gray):
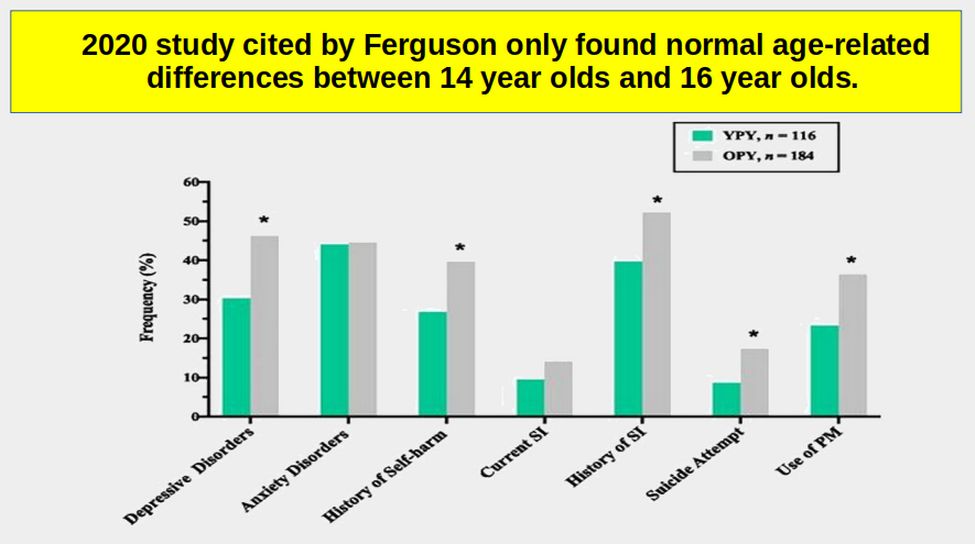
In short, 16 year olds suffered from more Depression but had about the same anxiety disorders as 14 year olds. So where did the misleading Ferguson claim come from? The answer is that it was referring to the fact that the study also did a statistical process called a logistic regression analysis. The result of the regression analysis was reported as follows:
“Late pubertal youth were 5.49 (95% confidence interval [CI]: 1.14–26.32) times and 4.18 (95% CI: 1.22–14.49) times more likely to report depressive and anxiety disorders, respectively, compared with early pubertal youth.”
While this appears to match what Ferguson wrote in his brief, he fails to report the most important fact (lying by omission). The omitted fact is the 95% confidence level is extremely wide. For example for depressive disorders, the range includes all values from a ratio of 1.14 to a ratio of 26.32. With a range this wide, the result is almost meaningless.
Yet Ferguson uses this nearly meaningless study to justify giving gender mutilation drugs to 12 year olds.
Later in the study, the authors admit that other things might explain the result. For example, they state that “ The prevalence of pediatric depression increases with age (25) and peaks after the onset of puberty (26).
25 Perou R, Bitsko RH, Blumberg SJ, et al; Centers for Disease Control and Prevention (CDC). Mental health surveillance among children—United States, 2005–2011. MMWR Suppl. 2013;62(2):1–35
26 Thapar, Collishaw, Pine, Thapar. Depression in adolescence. Lancet. 2012;379(9820):1056–1067
Neither of these links is very helpful. But since I have a Masters Degree in Child Development and have spent years studying this problem of Depression in teenagers, I will explain what is actually happening.
We have known for at least 50 years that mental health problems in teenagers increase with age. In short, these problems have nothing to do with being transgender or starting taking gender mutilation drugs. They have to do with being a teenager. Below is a chart from the CDC from a recent study: https://www.cdc.gov/childrensmentalhealth/data.html
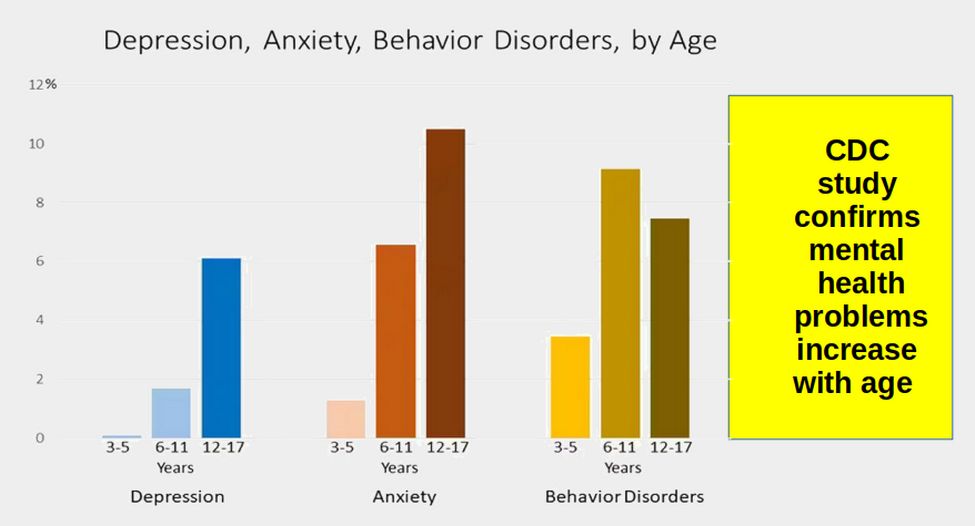
Most parents of teenagers have also observed this as they wonder what happened to their normal child who suddenly went crazy when they became a teenager. But this does not mean teenagers need a pile of toxic drugs. What they may need is mental health counseling such as CBT (Cognitive Behavior Therapy).
Thankfully, on August 21, 2023, the 11th Circuit Court of Appeals ruled against Bob Ferguson and in favor of the right of the state of Alabama to protect their children from gender mutilation drugs. Here is a link to their 59 page opinion. https://media.ca11.uscourts.gov/opinions/pub/files/202211707.pdf
Here is a quote from their decision: “States have a compelling interest in protecting children from drugs, particularly those for which there is uncertainty regarding benefits, recent surges in use, and irreversible effects… these medications can cause loss of fertility and sexual function.”
Gender Confusion is best treated with Counseling not Drugs
Hundreds of scientific studies support the conclusion that counseling for underlying mental health issues such as depression, anxiety, and emotional trauma should be the first line of treatment for children who are confused or distressed about their sex. Counseling for both the child and family, was once and is increasingly again recognized as the standard of care for minors with gender dysphoria. Giving kids toxic drugs does not address mental health issues or trauma issues or reduce suicides. There are better mental health alternatives to gender mutilation drugs which address underlying issues, rather than dodging them. There are more effective ways with better long term outcomes to deal with gender confusion than the chemical sterilization and surgical mutilation of healthy young bodies.
Estimate of number of children being harmed by Gender Transition Child Abuse in Washington State
10 years ago, there were only two gender transition clinics in Washington State. Currently, there are now more than 70 Gender Transition clinics in Washington state. Some clinics currently are transitioning (abusing) as many as 800 children. Here is an example of the growth of children harmed annually at a single clinic in Portland Oregon in the past 10 years:
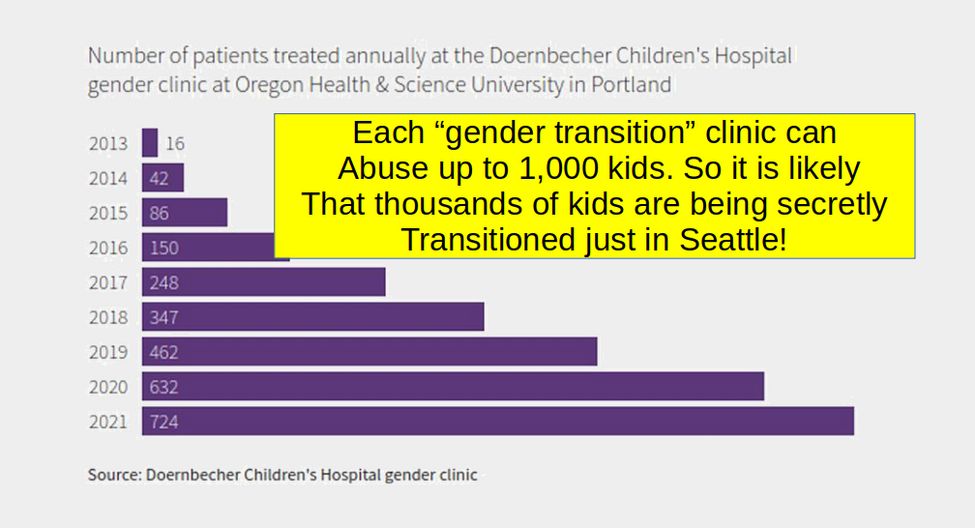
Therefore, as many as 70 times 800 or 56,000 children are being subjected to gender transition abuse here in Washington State. Another way to estimate the number of children harmed in our state by gender mutilation drugs is to multiple the number of high school students by the reported rate of Trans students per either the CDC or Gallup surveys. Both surveys conclude that about 20% of high school students have been brainwashed into joining the Trans Gender cult. Since we have about 300,000 high school students, 20% times 300,000 is an estimate of 60,000 students in the Trans Gender Cult Club in Washington state.
Estimate of the cost of harming 60,000 children with Gender Mutilation drugs in Washington State
The cost of gender mutilation drugs for a single child for a single year is about $40,000. The treatment typically goes on four 10 years. Surgery adds another $100,000 and cancer treatment can range from $100,000 to $500,000 total cost (with most paid for by tax payers). But skipping the cancer treatment, the cost will be at least a half million dollars per child. Multiply a half million times 60,000 students and the total cost is 30,000 million dollars or about $30 billion for ten years or about $3 billion per year just here in Washington state. Nearly all of this cost is paid by tax payers.
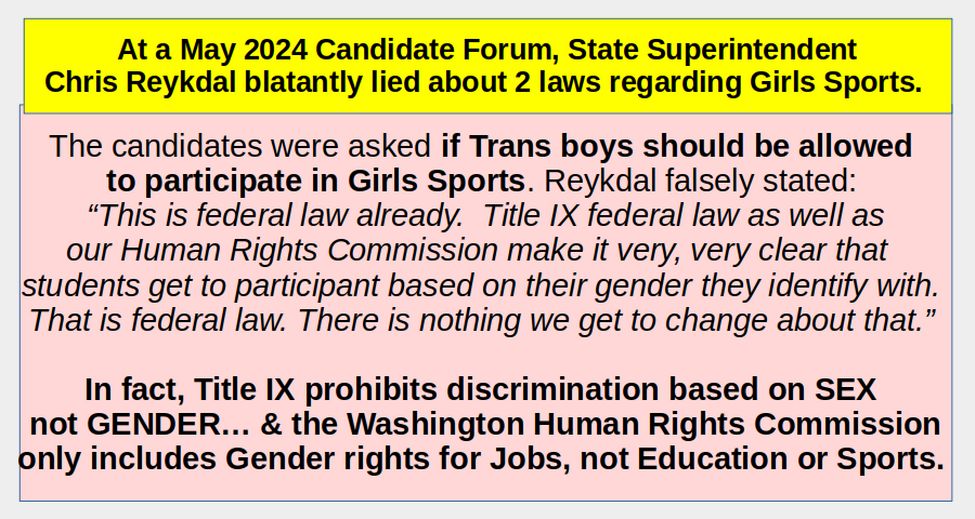
In summary, the lies told by Bob Ferguson and Chris Reykdal to promote drugging and severely harming tens of thousands of kids by pushing the Gender Mutilation Drug racket is robbing $3 billion per year from us tax payers and giving it to billionaires like Bill Gates that own both the drug companies and corrupt politicians like Bob Ferguson and Chris Reykdal.
This report is divided into 25 sections
Hopefully, you now have a better understanding on the kind of lies and fake science being used by Snake Oil Salesmen like Bob Ferguson and Chris Reykdal to promote giving toxic gender mutilation drugs to minors (often without their parents knowledge or consent). However, this is just the tip of a very ugly iceberg. In fact, the Gender Mutilation racket may be one of the worst crimes ever committed. As you read each of these 25 sections, you may and should get angry at the harm Ferguson and Reykdal are inflicting on innocent children. But please do your best to channel your anger into positive action. Help us replace Reykdal and Ferguson with people who actually care about the well being of our children.
In the following 25 sections, we will go further into both the science and politic corruption underlying the Gender Mutilation Racket:
1 Lies about Child Gender Transitions (Mutilations)
2 Why Gender Transition is an extreme form of Child Abuse
3 Why Minors can not give informed consent
4 Gender Dysphoria related to environment rather than genetics
5 Adverse Child Events underlying Gender Dysphoria
6 Social Media in the Development of Gender Dysphoria
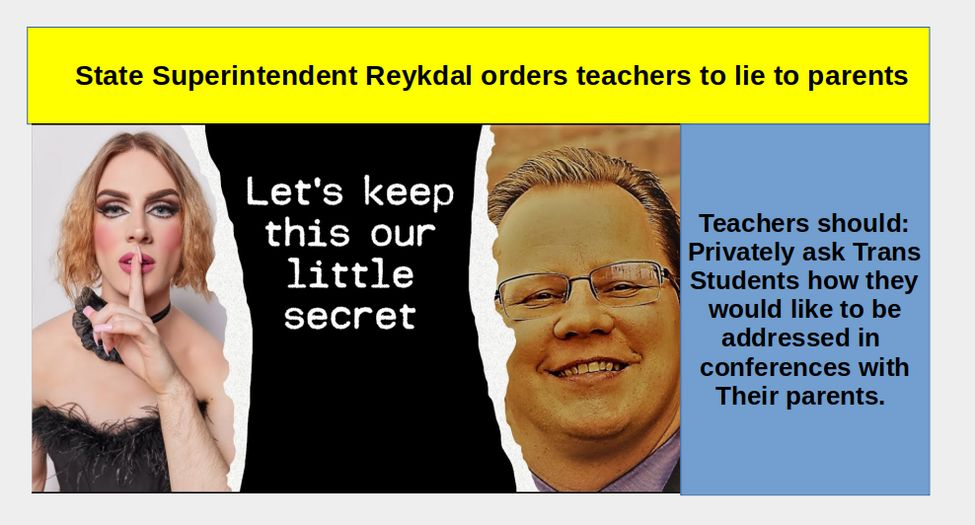
7 State Superintendent Reykdal orders teachers to lie to parents
8 La Center School District threatened for telling parents the truth
9 Consequences of Teachers Lying to Parents
10 Who is making money from this monstrous child abuse?
11 Senate Bill 5599 Eliminates Parental Notice
12 Backlash against SB 5599 led to the Parents Rights Initiative
13 May 2024 Legal Challenge to the Parents Rights Initiative
14 State Superintendent Reykdal blocks Parents Rights Initiative
15 Federal Health Centers put in schools to avoid parental notice
16 Washington laws promoting Gender Mutilation of Minors
17 US Supreme Court ruling on Parents Rights
18 Exposing WPATH Crimes against children
19 Inside the Gender Mutilation Scam Industry
20 Rapid Onset Gender Dysphoria
21 Florida judge rules gender mutilation is safe and effective
22 King County Judge Rules Against Parental Notification
23 Supreme Court to review state bans on gender mutilation
24 Resolution Opposing Giving Gender Mutilation Drugs to Minors
25 Four Steps to protect our kids from state child abuse
1 Lies about Child Gender Transitions (Mutilations)
There is a propaganda war being waged against parents and children by people making millions of dollars spreading monstrous lies. The biggest lie is for an authority figure, such as a teacher, to tell a child they can magically change their sex simply by changing the pronouns they use. Then to add insult to injury, for this same teacher to undermine the parent-child relationship by telling the child they must not tell their parent of their new “gender identity.” The fact is that it is not possible for anyone to change their biological sex. Instead, convincing a child to go down this path is likely to lead the child to a broken life of misery, cancer and early death.
Here are 6 of the biggest lies of the Gender Mutilation Industry.
Lie #1 Some children are born with the wrong sex and need to be given drugs to mimic their preferred gender.
FACTS: Science shows that while about 1% of children are not happy with their biological sex, more than 90% of these children outgrow this feeling by the time they reach adulthood. The remaining 10% suffered from serious mental health problems PRIOR to their gender concerns. Gender concerns are therefore a symptom of an underlying mental health problem – not a condition to be “fixed” with drugs. https://www.frontiersin.org/journals/psychiatry/articles/10.3389/fpsyt.2021.632784/full
Lie #2 Giving kids gender drugs restores their happiness
FACTS: There is no research that giving kids drugs improves their happiness over time. Gender mutilation advocates are quick to point out that when people who want gender drugs do not get them, they suffer a 40% risk of attempting suicide suicide 40%. What they fail to mention is that people who want gender drugs and do get them have a 42% risk of attempting suicide. So if anything giving kids gender drugs increases their risk of attempting suicide. Instead of giving troubled kids expensive ineffective experimental drugs, addressing their underlying mental health problems through counseling is what leads to long term happiness. Giving a child experimental drugs simply leads them down a path to a life of misery. See page 18 of this study: https://williamsinstitute.law.ucla.edu/publications/suicidality-transgender-adults/
Lie #3 Giving kids gender drugs is safe
FACTS: In 2019, a study was published of more than 3,000 minors given hormone drugs. The study confirmed that the risk of breast cancer rose 46 times (4,600 percent) in minors subjected to trans hormone drugs. https://www.bmj.com/content/bmj/365/bmj.l1652.full.pdf
The study and several others that found similar risks has led many countries including Sweden and Great Britain to move away from promoting gender drugs to banning giving them to minors.
Lie #4 Parents do not know about or care about their children
FACTS: The vast majority of parents care about their children and know more about their children that any teacher or other state worker. Parents should assumed to be good caregivers and should not have to fear the state kidnapping or brain washing their kids as a result of attending school. It is not parents we should worry about abusing children. Instead, it is the state that is abusing our children with experimental drugs.
Lie #5 A troubled child should be told to lie to their parents
FACTS: There is almost nothing one can do that is more harmful to a child than to tell them that their parents can not be trusted or that they need to lead a “double life” of lying to their parents when they are at home and constructing an alternate identity at school. It is not parents we should distrust. It is the drug industry that makes millions of dollars by convincing children that their snake oil will bring the child happiness.
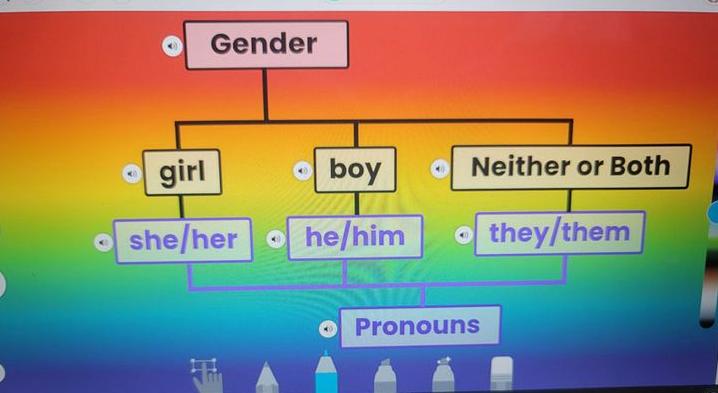
Lie #6 It is only polite to encourage a five-year old child to use a series of made-up pronouns rather than their real pronouns
FACTS: Forcing children to use a series of made up alternate genders and confusing pronouns leads children to needless doubt and fear – both harmful to learning and brain development - at a time when children should be focused on learning to read, write and do basic math.
Four Steps to Brainwash Kids
Brainwashing Step 1 Encourage children to use fake pronouns
The brain washing begins with stories about gay role models as soon as Kindergarten. Here is an image of an assignment given to First Graders asking them to magically choose from among several gender options:
Brainwashing Step 2: Normalizing gender mutilation by bringing in drag queens to First Grade classes
NYC spent more than $200k sending drag queens into schools to read to kids as young as THREE - sometimes without parental consent. In 2022 alone, Drag Story Hour made 49 appearances at 34 public schools.
Brainwashing Step 3: Encourage kids to take Trans hormones
Looks like a lot of fun, doesn’t it? Note that there is no mention that the Gender Hormones will cost the family or state tax payers $40,000 each year for 5 to 10 years and greatly increase the risk of cancer.
Brainwashing Step 4: Promote Sex Change Surgery
Sadly, even after all this money spent trying to change a person’s sex, the person is still left with the underlying mental health problems that led to the compulsion to change their sex in the first place.
End Result: Cancer Treatment
Even sadder, all of the experimental drugs are highly likely to lead to both cancer and an early death.
No rational adult would want any child to go down such an expensive, unhappy and deadly road.
Distortions of Science
The debate over the harm of gender mutilation is currently being played out in state legislatures and federal courts. 26 states have banned gender mutilation of minors while 14 states (including Washington state attorney general Bob Ferguson) have submitted court filings in favor of gender mutilation. Several federal judges have ruled in favor of state laws banning gender mutilation of minors. On August 21, 2023, one of the most significant federal court rulings was a 59 page decision by a three judge panel who agreed that Alabama has a rational basis for banning gender mutilation of minors in their state. The case was called Eknes-Tucker v. Governor, State of Alabama https://media.ca11.uscourts.gov/opinions/pub/files/202211707.pdf
Here are some quotes from this decision:
“There is no binding authority that indicates that the general right to "make decisions concerning the care, custody, and control of [one's] children" includes the right to give one's children puberty blockers and cross-sex hormone treatment.
Several studies demonstrate that hormonal and surgical interventions often do not resolve the underlying psychological issues affecting the individual. For example, individuals who undergo cross-sex cosmetic surgical procedures have been found to suffer from elevated mortality rates higher than the general population. They experience significantly higher rates of substance abuse, depression, and psychiatric hospitalizations. Minors, and often their parents, are unable to comprehend and fully appreciate the risk and life implications, including permanent sterility, that result from the use of puberty blockers, cross-sex hormones, and surgical procedures.
Alabama produced documents showing that public healthcare entities of Sweden, Finland, France, Australia, New Zealand, and the United Kingdom have raised concerns about the risks associated with puberty blockers and cross-sex hormone treatment and supported greater caution and/or more restrictive criteria in connection with such interventions. “
In response to this Alabama ruling, a group of doctors making millions of dollars pushing gender transition drugs on kids issued a 30 page report claiming that the three federal judges did not use “accurate science.” Here is a link to their report:
https://medicine.yale.edu/lgbtqi/clinicalcare/gender-affirming-care/report%20on%20the%20science%20of%20gender-affirming%20care%20final%20april%2028%202022_442952_55174_v1.pdf
Their report claims that gender altering drugs and surgeries are “safe and effective.” We will provide studies showing that the drugs are not safe - as they often lead to cancer and other health problems. Here we will look at their claim that gender drugs (hormones) are effective. After 10 pages of propaganda and unsupported claims, the discussion claims on page 11: “40% of trans individuals who do not receive hormones will attempt or complete suicide in their lifetime.”
The implication of this claim is that if we do not give trans kids hormone drugs, 40% of them might wind up committing suicide. To support this shocking claim, the report links to a study published in 2019 at this link:
https://williamsinstitute.law.ucla.edu/publications/suicidality-transgender-adults/
This data comes from an online self report – which is not exactly scientific. The 2015 U.S. Transgender Survey was an online survey of transgender adults, ages 18 and over, which was fielded in August and September of 2015. The 27,715 respondents came from all 50 US states.
There were huge problems with this report. For example, the median age was 26 compared to the US median age of 38. Also, there were a huge number of respondents reporting to be 18 years old which was the minimum age required to fill out the report. This indicates that many younger people filled out the report and lied about their age – claiming they were 18 when they were really younger than 18.
Also the percentage of white adults in the report was 82% which is much higher than the actual percentage of white adults in our population which is 62%. Finally, median household income was reported to be $35,000 when actual median household income that year was $56,500. Ignoring these glaring problems, scroll down to page 18 and read Table 4.
It does indeed indicate that: 41% of trans individuals who want hormones and do not receive hormones will attempt or complete suicide in their lifetime. However, in the very next line, it indicates that those who wanted hormones and have had them reported a lifetime suicide rate of 42%
Please read the above sentence ten more times and let it sink it. The authors of the so-called science based report assumed that we would not read the actual study – which indicates the exact opposite of what the gender – mutilation pushing doctors are claiming. It is bad that 40% of trans individuals who do not receive hormones attempt to commit suicide. However, it is much worse that 42% of trans individuals who do receive hormones will attempt to commit suicides. In other words, giving trans kids the hormones INCREASES their risk of committing suicide.
Also, in the same table it notes that “the lifetime attempted suicide rate for those wanting surgery but not getting was 41 percent while the lifetime rate for those wanting surgery and having gotten surgery was 40 percent. “
Put bluntly, the study these crooked doctors used to claim that drugs and surgery were effective concluded the exact opposite – that trans drugs and trans surgery are NOT safe or effective!
2 Why Gender Transition is an extreme form of Child Abuse
The American College of Pediatricians is a national organization of pediatricians and other healthcare professionals dedicated to the health and well-being of children. Their objective is to foster and stimulate improvements in all aspects of healthcare of infants, children, and adolescents. They have issued a 20 page report summarizing 55 scientific studies on the drawbacks of gender transitioning minor children. You can download and read their report at this link: https://acpeds.org/assets/imported/corrected-REVISED-NOV-2018-Gender-Dysphoria-in-Children-1.pdf
From a purely scientific standpoint, humans possess a biologically determined sex. The brains of all male infants are masculinized prenatally by their own endogenous testosterone, which is secreted from their testes beginning at about eight weeks’ gestation. There are literally hundreds of differences between male and female development. For example, serotonin levels in the male brain are 10 to 20 times higher on average than serotonin levels in the female brain. It is not possible to change a person’s genes through hormones or surgery. Sex change is objectively impossible.
The current scientific term for children who may be unhappy with their biological sex is called Gender Dysphoria (also called GD). It is estimated that this condition is rare – occurring in less than one percent of all children. Even then, among children who are clinically diagnosed as suffering from Gender Dysphoria, the condition resolved itself in about 90% of all cases without any medical intervention. For example, a 30 year study of 139 young biological boys who suffered from GD found that only 17 or 12% still suffered from GD when they were adults. The remaining 122 or 88% no longer had any problem with their biological sex. Here is a link to this study: https://www.frontiersin.org/journals/psychiatry/articles/10.3389/fpsyt.2021.632784/full
Thus, at most, this condition is a long term problem for less than one in one thousand students. Therefore, forcing all young students to be exposed to such a damaging life-altering treatment means that at least 999 of these students will run the risk of being harmed – and even the one in a thousand students that might benefit from gender transitioning will be subjected to serious harm as described next.
Consequences of Sex Mutilation Drugs
When children are given drugs to alter their appearance, the use of gonadotropin releasing hormone (GnRH) agonists followed by cross-sex hormones results in the sterility of minors. In addition, GnRH agonists arrest bone growth, decrease bone accretion and prevent the sex-steroid dependent organization and maturation of the adolescent brain.
In 2019, a study was published of more than 3,000 minors given hormone drugs. The study confirmed that the risk of breast cancer rose 46 times (4,600 percent) in minors subjected to trans hormone drugs.
https://www.bmj.com/content/bmj/365/bmj.l1652.full.pdf
Oral estrogen administration to boys also places them at risk for experiencing thrombosis/thromboembolism, cardiovascular disease, weight gain, elevated blood pressure, decreased glucose tolerance and gall bladder disease.
Negative Impact of sex reassignment surgery in adults
Surveys suggest that transgender adults initially express a sense of “relief” and “satisfaction” following the use of hormones and sex reassignment surgery (SRS). In the long term, however, SRS does not result in a level of health equivalent to that of the general population. Instead GD encouraged youth will face a transgender adulthood which will predispose them to certain morbidities and an increased risk of early death. For example, a 2001 study of 392 male-to-female and 123 female-to-male transgender persons found that 62 percent of the male-to-female (MtF) and 55 percent of the female-to-male (FtM) transgender persons were depressed. Nearly one third (32 percent) of each population had attempted suicide. A thirty-year follow-up study of post-operative transgender patients from Sweden found that thirty years out from surgery, the rate of suicide among post-operative transgender adults was nearly twenty times greater than that of the general population.
See Cecilia Dhejne, et al., Long-term Follow-up of Transsexual Persons Undergoing Sex Reassignment Surgery: Cohort Study in Sweden, (Feb. 22, 2011) https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0016885
As the following chart shows, adverse outcomes including death occurred throughout the follow up period.
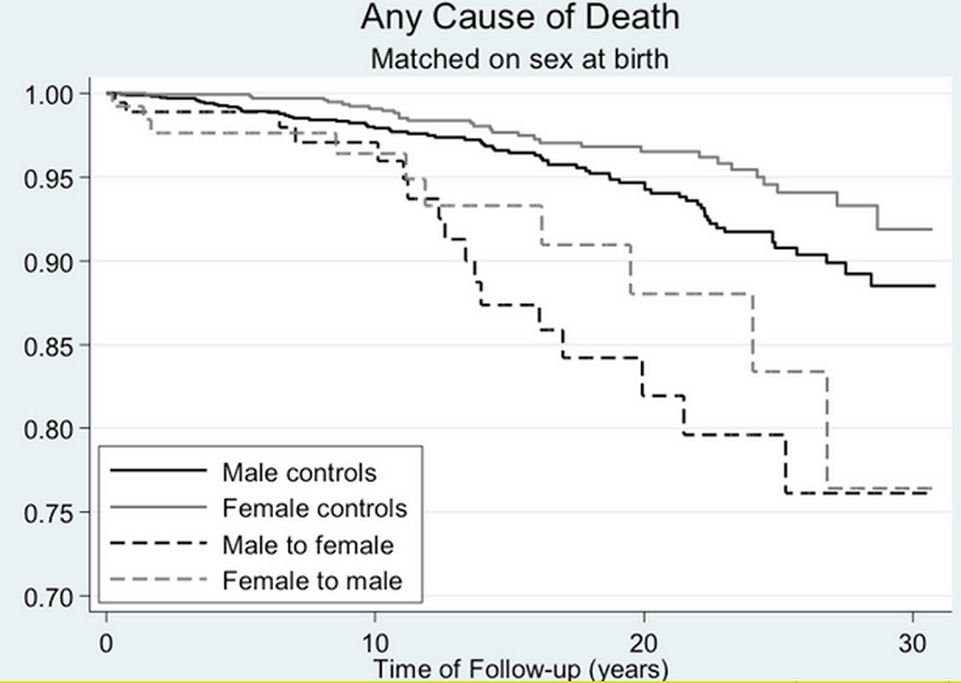
Below is a table of adverse outcomes compared to normal controls:
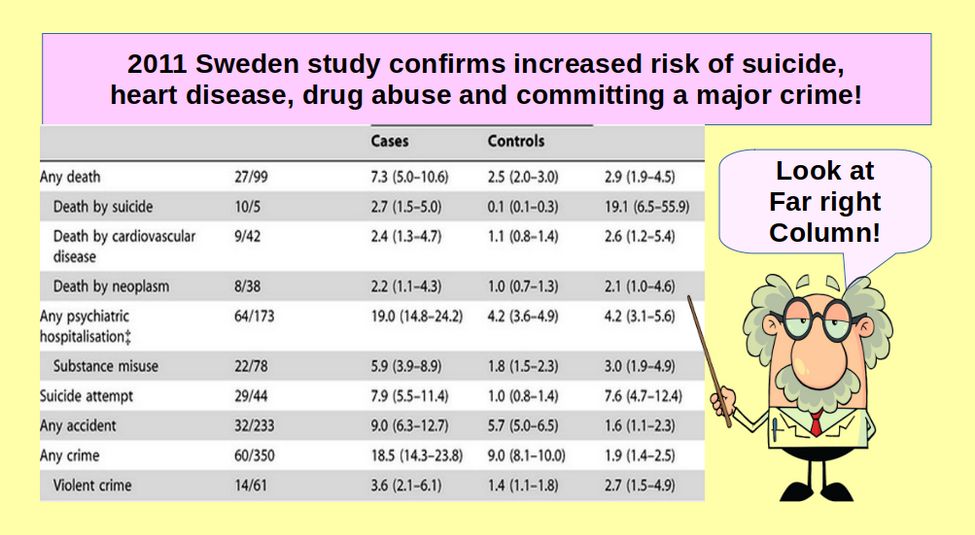
Look at the far right column in the above table to see the risk ratio for transgender adults compared to control adults. For example, those who had gender mutilation surgery were 3 times more likely to abuse drugs or commit a violent crime. No rational caring person would approve of sending any child down such a horrible path.
Texas Attorney General issues opinion that Gender Transition is Child Abuse
On February 18, 2020, Texas Attorney General Ken Paxton released a formal legal opinion concluding that performing certain “sex-change procedures” on children—including surgeries, cross-sex hormones, and puberty blockers—constitutes child abuse under Texas law. https://texasattorneygeneral.gov/sites/default/files/global/KP-0401.pdf
“You ask whether the performance of certain medical and chemical procedures on children—several of which have the effect of sterilization—constitute child abuse. You specifically ask about procedures falling under the broader category of “gender reassignment surgeries. Additionally, you ask whether “providing, administering, prescribing, or dispensing drugs to children that induce transient or permanent infertility” constitutes child abuse.”
“These procedures and treatments can cause “mental or emotional injury to a child that results in an observable and material impairment in the child’s growth, development, or psychological functioning. These procedures and treatments can cause a physical injury that results in substantial harm to the child. Based on the analysis herein, each of the “sex change” procedures and treatments enumerated above, when performed on children, can legally constitute child abuse.”
3 Why Minors can not give informed consent
Minors cannot give informed consent because children have developing and immature brains, their minds change often, they are prone to risk-taking, they are vulnerable to peer pressure, and they don’t grasp long-term consequences. The adolescent brain’s prefrontal cortex is immature and is limited in its ability to strategize, problem solve and make emotionally laden decisions that have life-long consequences. In females, the prefrontal cortex is not fully developed until about age 20. In biological males, the prefrontal cortex is not fully developed until about age 25 – which is why some young men make very poor decisions and tend to be risk takers. They simply do not yet have fully developed brains.
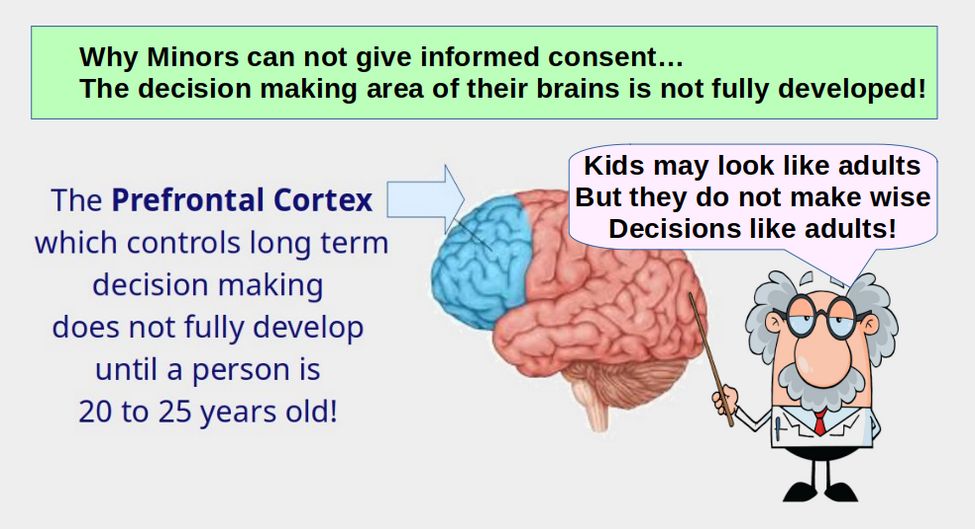
Final brain maturation begins during adolescence with the prefrontal cortex (that part of the brain associated with high-level reasoning, executive function, weighing of consequences, planning, organization, emotional regulation, and rational decision-making) being among the last to mature.
This is why young adults are more likely to get speeding tickets and car accidents than older adults – a fact well known by car insurance companies. This is also why adolescents are more affected by the influence of peers, less future oriented, more impulsive, and differ in their assessment of risks and rewards compared with adults.
Here is a link to a report on adolescent brain development: https://publications.aap.org/pediatrics/article/146/Supplement_1/S18/34490/Adolescent-Brain-Development-and-Medical-Decision?autologincheck=redirected
4 Gender Dysphoria related to environment rather than genetics
Those who promote gender mutilation of minors claim that some children are “born in the wrong body”, that the condition is genetic and thus there is a need to transition the child into the correct gender. This claim is not supported by scientific research. Instead, it is well accepted that a child’s emotional and psychological development is impacted by positive and negative experiences from infancy forward. Family and peer relationships, one’s school and neighborhood, the experience of any form of abuse, media exposure, chronic illness, war, and natural disasters are all examples of environmental factors that impact an individual’s emotional, social, and psychological development.
The literature regarding the development of childhood GD suggests that social reinforcement, parental psychopathology, family dynamics, and social contagion, facilitated by mainstream and social media, all contribute to the development and/or persistence of GD. Sometimes parental psychopathology is at the root of the social reinforcement. For example, among mothers of boys with GD who had desired daughters, a small subgroup experienced what has been termed “pathologic gender mourning.” Within this subgroup the mother’s desire for a daughter was acted out by the mother actively cross-dressing her son as a girl. These mothers typically suffered from severe depression that was relieved when their sons dressed and acted in a feminine manner.
Coates and Person (1985), provided data on a high rate of separation anxiety disorder in boys with GD. These researchers argued that the high rate of separation anxiety could be accounted for by a great deal of familial psychopathology, which rendered the mothers of these boys unpredictably available. The emergence of separation anxiety preceded the first appearance of feminine behavior, which was understood to serve a representational coping function of recapturing an emotionally unavailable mother. A.S. Birkenfeld-Adams (1999)has shown a rate of insecure attachment to the mother, https://focus.psychiatryonline.org/doi/epdf/10.1176/foc.3.4.598
Green (1987) assessed the amount of shared time between parents of feminine boys and control subjects during the first 5 years of life. The fathers of feminine boys reported spending less time with their sons from the second to the fifth year than did the fathers of control subjects. The mothers of feminine boys also reported spending less time with their sons than did the mothers of control subjects.
For girls with GD, the mother–daughter relationship is often filled with unresolved conflict, leading to the daughter not identifying with the mother. In some instances, femininity is devalued and masculinity is overvalued, which seem to be encouraged by the parents. Furthermore, there have been cases in which girls are afraid of their fathers who may exhibit volatile anger - including abuse toward the mother. A girl may perceive being female as unsafe, and psychologically defend against this by feeling that she is really a boy; subconsciously believing that if she were a boy she would be safe from her father.
It has also been found that among children with GD, the rate of maternal psychopathology, particularly depression and bipolar disorder is “high by any standard.” Additionally, a majority of the fathers of GD boys are easily threatened, exhibit difficulty with affect regulation, and possess an inner sense of inadequacy. These fathers typically deal with their conflicts by overwork or otherwise distance themselves from their families. Most often, the parents fail to support one another, and have difficulty resolving marital conflicts. This produces an intensified air of conflict and hostility. In this situation, the boy becomes increasingly unsure about his own self-value because of the mother’s withdrawal or anger and the father’s failure to intercede. The boy’s anxiety and insecurity intensify, as does his anger, which may all result in his inability to identify with his biological sex.
The core symptoms of gender dysphoria in childhood rarely exist in isolation. Severe psychopathology preceding the onset of GD is common. In a study of 47 adolescents seeking GD treatment, 75% (35/47) had been or were currently undergoing child and adolescent psychiatric treatment for reasons other than gender dysphoria when they sought referral. 64% (30/47) were having or had had treatment for depression, 55% (26/47) for anxiety disorders, 53% (25/47) for suicidal and self-harming behaviors. 68% (32/47) had their first contact with psychiatric services due to other reasons than gender identity issues. https://capmh.biomedcentral.com/articles/10.1186/s13034-015-0042-y
5 Adverse Child Events underlying Gender Dysphoria
Adverse Childhood Events (ACEs) refer to a range of negative situations a child may face or witness while growing up, such as physical neglect, parental separation or divorce, living in a household in which domestic violence occurs, or living with an alcoholic. These experiences negatively alter the brain at a deep level where most basic needs originate and a person’s identity is formed. Because there is a known and strong relationship between Childhood Mental Health problems such as anxiety, depression and detachment, and a relationship between these problems and GD, there is almost certainly a relationship between adverse child events, including sexual abuse, and the development of gender confusion.
Trauma in childhood is known to impact child development and the occurrence of mental health problems later in life, and research shows that mental illness precedes the onset of transgender ideation in young people. This suggests that gender distress is not the problem—mental illness is. For example, a major 2018 study of mental health in transgender-identifying youth found overwhelming evidence that mental illness is present before the onset of transgender belief. This study compared over 1,300 trans-believing youth with age-matched peers using clinical data gathered from three large pediatric practices in California and Georgia. Psychological disorders such as anxiety, depression, and attention deficit disorders were several times higher than the peer group, suicidal ideation was up to 54 times higher, and self-harm was up to 144 times higher. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5914494/pdf/PEDS_20173845.pdf
According to Dr. André Van Mol—the co-chair of the American College of Pediatricians’ Committee on Adolescent Sexuality —in the overwhelming majority of cases, the desire to switch one’s gender identity is closely connected to adverse experiences in childhood. More broadly, studies have reported a high frequency of childhood emotional and physical neglect and abuse among transgender-identifying individuals. Given the role of ACEs play in the development of gender dysphoria. it is adding insult to injury to advocate that the first and only step in treating trauma done to a child’s identity is to alter their body with cross-sex hormones and surgery. By not addressing the underlying causes of the problem, gender altering treatments are not merely ineffective, they are ch. They are child abuse.
6 Social Media in the Development of Gender Dysphoria
A recent study documented an increasing trend among adolescents to self-diagnose as transgender after binges on social media sites such as Tumblr, Reddit, and YouTube. In on-line forums, parents reported that their children seemed to experience a sudden or rapid onset of gender dysphoria, appearing for the first time during puberty or even after its completion. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0202330
Parents describe that the onset of gender dysphoria seemed to occur in the context of belonging to a peer group where one, multiple, or even all of the friends have become gender dysphoric and transgender-identified during the same time frame. Parents also report that their children exhibited an increase in social media/internet use prior to disclosure of a transgender identity. In many schools and communities, there are entire peer groups “coming out” as trans at the same time.
Parents reported subjective declines in their child’s mental health (47.2%) and in parent-child relationships (57.3%) since the child “came out” and that their child expressed a range of behaviors that included: expressing distrust of non-transgender people (22.7%); stopping spending time with non-transgender friends (25.0%); isolating themselves from their families (49.4%), and only trusting information about gender dysphoria from transgender sources (46.6%).
Most (86.7%) of the parents reported that, along with the sudden or rapid onset of gender dysphoria, their child either had an increase in their social media/internet use, belonged to a friend group in which one or multiple friends became transgender-identified during a similar time frame, or both. This suggests that social peer influences may be at play in the rapid growth of GD students.
7 State Superintendent Reykdal orders teachers to lie to parents
Washington State Superintendent has a long history of ignoring science on everything from masks and PCR tests to school closures. Due to his utter lack of research, children in Washington state have been harmed more than any other children in the nation. It should therefore not be surprising that Reykdal has ignored the scientific research on gender mutilation. Instead, he has insisted on brainwashing teachers and children with some shocking mandatory regulations which you can read at this link:
https://ospi.k12.wa.us/policy-funding/equity-and-civil-rights/information-families-civil-rights-washington-schools/gender-inclusive-schools
His radical new policies, launched in January 2020, begin by falsely claiming that some sort of unspecified federal laws require schools to lie to parents in order to protect the gender change “choices” of children. Elsewhere in this report, we review the current federal laws and recent court decisions. In short, while the rights of parents are firmly established, the right of a 5 year old to make major decisions about anything do not exist. But Reykdal has a long history of lying when it comes to rationalizing any agenda he is in favor of.
Here are just a few of Reykdal’s insane policy mandates:
Students have the right to be addressed by their requested name, pronoun (e.g., he/him, she/her, they/them, etc.), and gender designation.
Public schools must allow students to use the restroom that corresponds to their gender identity.
Public schools should provide access to the locker room that corresponds to a student's gender identity.
Public schools must allow all students to participate in physical education and athletics that correspond to their gender identity.
A designated school employee should offer to meet with a student who is transgender, either upon the student’s enrollment or when there’s a change to an enrolled student’s gender identity or expression. During that meeting, the designated school employee should:
Consult with the student about their preferences for family involvement, in advance of contacting the student’s parents or guardians.
Privately ask the student how they would like to be addressed in class, in correspondence sent home, and in conferences with their parents.
In short, the student is encouraged to lie to their parents.
Parents Rights… What information about a student’s gender can a school share with their parents or guardians?
It depends. Federal and state privacy laws protect personally identifiable student information from unauthorized disclosure. The federal Family Education Rights and Privacy Act (FERPA) gives parents and legal guardians the right to request their student’s education records, and if requested, the school district will provide those records to the parent or legal guardian. Education records can include grades, transcripts, class lists, student course schedules, health records, and student discipline files.
OSPI is not aware of any applicable federal or state law that requires a local education agency (LEA) to affirmatively disclose a student’s gender identity to their parents or legal guardians. LEAs should not disclose a student’s gender identity to others, including their parents or legal guardians, unless the student authorizes the disclosure or the disclosure is required by law, such as when a parent or legal guardian requests the student’s education record under FERPA.
In short, teachers are required to lie to parents.
Students who identify as transgender or gender-expansive may wish to transition socially and/or medically. Social transition may include changes to a person’s name, pronouns, clothing, hairstyle, behavior, mannerisms, and choice of activities. Medical transition may include medications used for hormone therapy or gender affirming surgeries. Transitioning either socially or medically is a personal decision. In all cases, Washington’s public schools have a civil rights obligation to treat students consistently with their gender identity and gender expression at school.
Are classroom lessons on gender age-appropriate?
Yes. Starting this school year, all public schools must provide comprehensive sexual health education (CSHE) to all students consistent with the Health Education K–12 Learning Standards. Washington state law requires CSHE to be “medically accurate, age appropriate, and inclusive of all students” for students in grades 4–12. State law makes clear that the only CSHE requirement for students in kindergarten through third grade is instruction in Social Emotional Learning.
Here are some quotes on how school districts are implementing Reykdal’s WOKE agenda:
Educators are going much farther than teaching gender identity to Kindergarteners. They’re actively withholding information from parents about a student’s purported gender identity. This isn’t merely dangerous; it’s keeping families apart. Schools in Washington are either adopting or implementing policies that keep parents in the dark. Educators and administrators will not reveal gender identity, different names a student may adopt, and even mental health concerns that could help parents connect their child with objective mental health experts. In some cases, they’re ignoring direct instructions from parents.
An updated policy in the Puyallup School District instructs staff to have secret meetings with students it believes to be transgender. A Northshore District school keeps detailed records on students, informing teachers what pronouns or names to use when talking to their child’s parents. In Bellingham, the superintendent endorses a worksheet teachers use to ask students what secret name and personal pronouns they prefer to be kept from parents.
The Puyallup School District recently updated its Gender Inclusive School policy. It encourages staff to meet with transgender students in secret to come up with ways to keep information away from parents at the student’s request. The policy reads: “The principal or building administrator—or an appropriate, designated school employee—is encouraged to request a meeting with a transgender or gender-expansive student upon the student’s enrollment in the district or in response to a currently enrolled student’s change of gender expression or identity. Before contacting a student’s parents, the school will consult with the student about the student’s preferences regarding family involvement and consider whether safety concerns are present for the student.”
The district’s policy knowingly lies to parents about their son or daughter, potentially driving a bigger and unnecessary wedge between them. Staff must “ask known transgender students how they would like to be addressed in class, in correspondence to the home, and at conferences with the student’s parent/guardian.”
“Before communicating with parents of transgender students, it’s important to ask the student how school employees should refer to the student when talking with their parents and guardians,” the policy states. “For parents who are not supportive, or who are not aware of the student’s transition at school, referring to their name and pronoun could be very dangerous. The district will not condone the intentional or persistent refusal to respect a student’s gender identity or gender expression, or inappropriate release of information regarding a student’s transgender status.”
The Central Valley School District (CVSD) in Liberty Lake, Washington, near Spokane, offered a presentation of its gender inclusivity policy Monday, during which time parents were not permitted to ask questions.Districts are tearing families apart, rather than strengthening them. Kids experiencing confusion over their gender are better off navigating their feelings with parents — not teachers who may have political agendas. Teachers will never truly love these kids as much as their parents. How do kids benefit by living two separate lives where they can’t be themselves in front of their parents? Loving mothers and fathers can help guide their kids and provide quality mental health professionals when necessary. But they can’t help if they don’t know. Teachers should help connect kids with parents, not encourage them to keep secrets.
The rationale for teaching 7 year olds about magical gender options.
The Edmonds School District developed lesson plans on self-identity that includes the claim that sometimes, gender does not exist. Other times, a person can have two genders. First graders learn about the “nonbinary experience” and teachers are told to ask students to list their gender identities so that “gender nonconforming” students can feel more comfortable.
Here is a link to the 125 page state standards:
https://ospi.k12.wa.us/sites/default/files/2023-08/hpe-standards.pdf
Under state guidelines, Washington public schools must provide age-appropriate lesson plans on a variety of sexual health topics. Under the theme of “self-identity,” kindergartners and first graders should learn “that there are many ways to express gender.” But the intent does not appear to be to promote the concept of gender identity because that topic is listed by the state as appropriate starting in the fourth grade.
Though the book publisher says it’s meant for a second-grade reading level, the Edmonds School District uses it for students in the first grade. In a note to teachers, the publisher says the book “helps normalize the idea that gender identity is fluid.”
The publisher explained that the lesson plans were based on state-mandated health standards.
“Teachers use the standards to design lessons to provide a variety of age-appropriate and grade-level learning,” she/her explained via email.
This isn’t age-appropriate. The mother was correct to question the curriculum. Neither gender identity nor the idea that gender doesn’t exist is appropriate for first graders. Not only is it false to claim gender doesn’t exist, but it would also obviously be confusing to 7-year-olds.
A teacher in Washington state who spoke with The Daily Wire broke down on the phone as she described how helpless she feels in the face of the new gender identity policies.
“You know, I love teaching and I love being with the kids and I’m thinking, I’m one of the last conservative teachers in my building. If I’m gone, there’s no one,” she said, her voice breaking. “There’s no one there that would tell them any kind of truth.”
Teachers at her school were told by school counselors to use students’ preferred pronouns and names without letting parents know, she said. Last year, this teacher said she made the mistake of calling up a parent and telling them their child wanted to adopt a new name and gender identity. She asked the parent whether that was okay. The parent responded along the lines of, “definitely not, we’re Christians,” and the teacher was pulled into the principal’s office and counselor’s office and reprimanded for divulging that information to the parent. At the beginning of this school year, that school made a point of spending time going over the OSPI guidelines on parental notification and gender identity with teachers in detail.
https://www.dailywire.com/news/washington-state-tells-teachers-to-hide-student-gender-transitions-from-parents
When a teacher tells her students to lie to their parents, or conceal information, there is something evil at work here. Harm is intended. We should never deceive ourselves into thinking that there may be some innocent explanation.
8 La Center School District threatened for telling parents the truth
In March, 2023, La Center school district officials got up the courage to openly oppose Reykdal’s insane policies. The district updated its "gender inclusive schools" policy to involve parents in all discussions about pronoun usage and restrict such conversations in the classroom.
Asking students their preferred pronouns, according to both the policy and district Superintendent Peter Rosenkranz, is an act of "facilitating questioning gender identity or to facilitate gender transitioning." "Curriculum, instruction, and 'Gender-affirming' activities in schools may cause gender-confusion for children," the policy reads under the "Guiding Principles" section.
Rosenkranz sent a staff email instructing teachers to not include a question about preferred pronouns in any getting-to-know-you surveys that teachers have students complete at the beginning of the school year.
In response, a complaint regarding the La Center School District policy was filed to the state Office of Superintendent of Public Instruction. Author of the complaint, Manny Santiago, the director of the state LGBTQ Commission, said language throughout the policy is dismissive and reflects a lack of understanding of what it means to be a member of the LGBTQ+ community.
The policy in question is titled 3211P, Procedure: Gender-Inclusive Schools.
At its core, the policy encourages district employees to abstain from any conversations about gender identity in the classroom, arguing that the role of the district is to provide academic education only.
According to state guidance, when a student asks their teacher if they may go by a specific set of pronouns, the teacher and school employees should honor that request. La Center's policy pushes against the guidance and, in one instance, contradicts itself.
Under a section titled "Collaboration Family Communication Protocol," the policy reads, "When a student requests being called by a different name or pronoun indicating a change in gender, we are to honor that request."
When such a request is made, however, the policy instructs staff to inform the principal and the student's counselor who then consult with the student to determine the nature of their home situation and how or if parents should be notified. If a parent asks the school whether their student has requested a name or pronoun change, the school will inform them.
In an interview, Rosenkranz said he would approach every family with the assumption that their intentions and home life are positive and that he and the district would ultimately adhere to the parents wishes for their child, even if they differ from the child's own.
"This is a more family-friendly approach. The state wants us to determine danger of parents, and that's not our role. I'm a mandatory reporter, not a mandatory judger," Rosenkranz said. "The part that folks are gravitating to are people talking to parents — our perspective is why would we deny our kids access to the No. 1 resource in their lives, their parents?
Most important, the state should not dictate policies to local school districts which are contrary to the wishes of the local community.
9 Consequences of Teachers Lying to Parents
One obvious consequence of Reykdal’s policy of forcing teachers to lie to parents is that parents no longer trust placing their precious children in the hands of abusive teachers. Tens of thousands of parents have pulled their kids out of public schools since Reykdal took office and radically changed our public school policies based on his Woke agenda. But many parents can not afford to take their kids out of public school. Here are just three of thousands of examples of the state-caused harm inflicted on children when the state and or school district forces teachers to lie to parents and when teachers encourage children to lie to their parents.
In Virginia, a mother is suing Appomattox County Public Schools after her daughter, who had secretly transitioned at school, ran away, was kidnapped by a sex trafficker and then raped repeatedly in a locked room in Baltimore.
In California, the Spreckels Union School District agreed to a $100,000 settlement with a local mother after she charged that the school staff “secretly convinced” her daughter that she was bisexual and transgender.
In Washington state, a family was forced to flee the country after a teacher attempted to secretly “transition” their 10 year old daughter https://www.city-journal.org/article/we-thought-she-was-a-great-teacher
Tia, a girl who was only 10 years old and going to an elementary school in Olympia Washington, had been convinced by her WOKE Fifth Grade teacher to magically change her gender at school.
Mrs. A is a committed advocate of gender ideology. In public, she praised the district for its absolutist LGBTQ policies, like one disallowing parents from opting their children out of Pride Month curricula. Mrs. A is an expert and manipulating the school data management system to hide information from parents about name and gender. In April, 2022, Mrs. A stood with Tia at the front of her class and told them that Tia had changed her name and pronouns. Her new name was Felix, her new pronouns were “he/him/they/them,” and no one outside school was to know. Tia’s parents couldn’t know. The other students in the class couldn’t tell their parents, either, for fear of one of them outing Tia to her parents.
But the school staff was made aware via an e-mail sent by Mrs. A announcing that Tia “has opened up to me and has just requested this change . . . This change is his right and is not to be questioned.”
The e-mail also instructed fellow staff not to change Tia’s information in the school’s “skyward” electronic database in order to ensure that the parents remained unaware. It was a secret between the children and the adults in their school, to be kept from their families.
“The girls would never be allowed to say her real name in front of Mrs. A because Mrs. A would correct them,” said Hammel. “Because of this, [Hammel’s daughter] stopped hanging out with Tia outside of school and on the playground. She didn’t know how to act.”
As her friends became increasingly confused and distant, Tia’s drawing lost its color. Pictures that were once vibrant turned black and white, her classmates said. And the already-quiet girl became even more reserved, wanting to talk only to Mrs. A. One day, the class went on a field trip to visit the local middle school. Tia’s mother came along to chaperone, and Tia told her class to call her by her old name for the day. But on the walk, Anne Crawford’s daughter accidentally called her Felix. “Her mom was confused and asked her to call Tia by her normal name,” Crawford said, as her daughter relayed the story in the background of our phone call. “It was very confusing for my daughter; she was wondering why the girl was lying to her mom.”
“A little bit later, in May, my daughter and a friend were both at the house working on a group project that Tia was also involved in,” Jess Davis recalled. “They were explaining each of their parts and when they got to the point of Tia’s part, my daughter suddenly didn’t know how to discuss her. She started doing this thing where she’d be looking up and would try to keep things straight, saying, ‘he, she, I mean . . . we are outside of school so, it’s she, but.’ She got to the point where she was hyperventilating. And I was watching this and just felt like, holy cow. “I stopped her and told her just to be kind and respectful,” Davis continued. “And I gave her permission not to participate in this.”
“No, Mom, we have to, or else we’ll get in trouble,” Davis’s daughter retorted, as her friend nodded. “You have to say it the right way.”
They both had tears in their eyes at this point,” said Davis. “And my daughter’s friend said, ‘and we’re not supposed to tell our parents.’ ”
The secret was being divulged, and parents were starting to hear that a child in their local elementary school had transitioned genders — seemingly all the parents except Tia’s were hearing it. But then Tia couldn’t handle it anymore. During Davis’ phone call with her at the ice cream social, Tia’s mother said that “her daughter had come to her and was crying and very upset. She was saying she wants to go to school, see her friends like normal, and doesn’t want to be a boy anymore. But Tia was afraid that Mrs. A would be mad at her and wouldn’t like her anymore. Her mom was like, ‘What are you talking about?’”
Tia’s mother had noticed the girl’s once-colorful art turning dark, Davis told me. “She wasn’t eating well. Her sleep was affected. She saw a dark cloud over her daughter, and her daughter wanted to talk only to Mrs. A, even at night and on weekends.”
So Tia’s mother decided to take Tia to school and confront Mrs. A. But as soon as Mrs. A realized that the mother knew, “Mrs. A stopped addressing the mom and started looking at the daughter and talking to her directly,” said Davis. “She asked Tia, ‘Are you OK? Do you need help?’ And the mom told her, ‘Stop talking to my daughter! Leave her alone!’ but Mrs. A wouldn’t acknowledge her.”
So Tia’s mother left the classroom and sought out the principal and school counselor. But the principal informed her that “Mrs. A had done nothing wrong and was just following school policies,” Davis explained. “They treated her like she was crazy and had no grounds.”
The mother took Tia home, bewildered after a troubling conflict with the people charged with educating her daughter. Tia and her younger brother were quietly driven out of the state, to a house in Oregon, where they stayed for a while before leaving the country.
“The family is very scared,” Davis said. “They were struggling and had no idea what to do. The dad just wanted to get away from everything and forget that it ever happened. There’s a lot of shame. And a lot of, ‘How could we let this happen to our child, and we didn’t know?’ ”
10 Who is making money from this monstrous child abuse?
The most obvious criminals are the drug companies that make gender transition drugs. These experimental drugs can cost $40,000 or more per child per year – often paid for by the tax payers. These drugs are given for 5 to 10 years. After taking these drugs, there are often surgeries which add another $100,000 to the cost. These drugs often lead to cancer, the treatment of which can be another $500,000 or more.
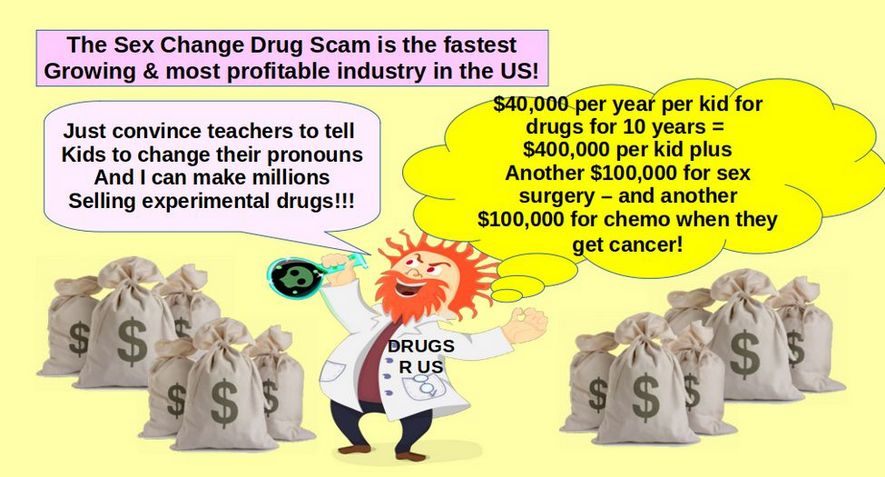
So the drug company and medical industry profit from each gender mutilated child can exceed one million dollars. This is why the Gender Mutilation racket is the fastest growing and most profitable medical practice in the US.
Drug companies and surgeons are not the only ones making a killing off convincing children to change their gender. The leading advertiser for all corporate media is the drug industry. So we are not likely to hear the truth from them. Also drug companies are a leading contributor to political campaigns. So few politicians will want to go up against the drug corporations.
A related question is who is paying for gender mutilation of minors?
There appears to be two payment pathways. The first is that those paying for health insurance as seeing a huge rise in monthly payments as states such as Washington have passed laws requiring health insurance providers to provide gender mutilation coverage.
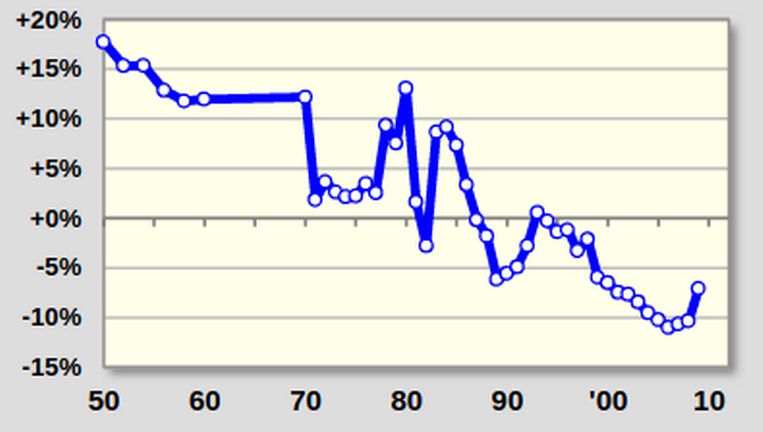
The second group are those who pay state and federal taxes as both state and federal funds are being used to pay for gender mutilation. Here is a graph of the increase in Pennsylvania:
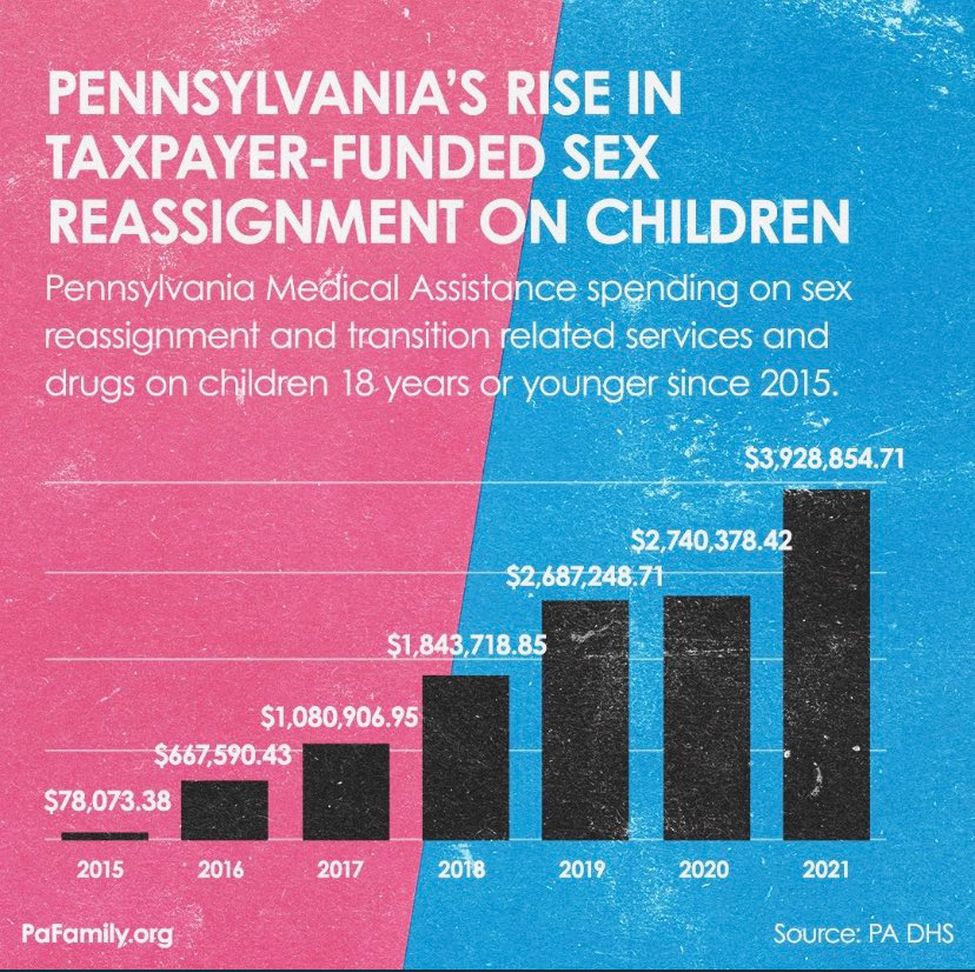
Thus, you are the one who is paying for the rise in gender mutilation.
11 Senate Bill 5599 Eliminates Parental Notice
In April 2023, the Washington State legislature passed Senate Bill 5599 which basically killed parents rights in Washington state. It was the first bill and worst bill in the history of the US to undermine the crucial relationships between children and their parents. https://app.leg.wa.gov/billsummary?BillNumber=5599&Year=2023&Initiative=false
Senate Bill 5599 allows the state to legally hide runaway children from their parents if the parents don’t consent to their child’s “gender transition” or abortion. No allegation of abuse in the household is required. The bill allocated $7.5 million of our taxpayers’ money to provide grants to school linked organizations to pay for gender transition and abortion procedures. During hearings on the bill in February 2023, more than 4,700 public comments were received, with 98% of them in opposition to the Gender Transition bill. Yet despite this massive opposition, the bill passed on a party line vote and became state law on July 23, 2023.
When SB 5599 received a hearing before the Senate Human Services Committee on Feb. 6, more than 4,700 people signed in with an opinion on the bill – and 98% were opposed, including parents from the LGBTQ community. One former transgender youth testified against SB 5599, sharing her experience as a sexual-assault survivor and her concern about the effects of the bill on vulnerable children. She said, “In the short term, I might have felt better having medically transitioned. Despite feeling better in the short term, medical transition would have profoundly damaged me, potentially even more than the sexual assault [that caused her gender dysphoria].”
Here are some of the comments opposing Senate Bill 5599:
“There is no mention about parents or parental involvement but rather an emotional response to helping children. The bill doesn't say how long youth can be away from home, this should be considered child abuse. A parents job is to protect their child, this bill strips parents of that ability. This bill legalizes the kidnapping of children. “
Senator John Braun wrote the following about the drawbacks of this bill: “Under Senate Bill 5599, children could disappear by simply claiming they are seeking what the bill calls “protected health services,” such as gender counseling or puberty-blocking chemicals. It clears the way for children between ages 13 and 18 to stay at these facilities without their parents’ knowledge for an indefinite time while seeking services related to gender dysphoria and gender transitioning… Like so many other health-related situations, gender dysphoria presents unique needs that deserve attention. But this should not mean removing parents from the decision-making process. This bill disenfranchises loving parents who deserve to have a say in the care of their teenage children. SB 5599 drives a wedge between vulnerable kids and their parents, at a time when a teen lacks the perception and judgment to make critical life-altering decisions.”
“A parent may not even know why the child ran away and could involve law enforcement or other groups in a desperate search – all the while going through an unnecessary emotional nightmare, imagining the worst about what might have happened. Unless there is reason to suspect parental abuse or harm, parents deserve to know where their teenagers are.
“Democrats have claimed many times that the brains of minors are not fully developed until age 22. It’s revealing how brain research matters to them when juveniles break the law, but not when they seek life-altering, potentially irreversible health care.”
Legal Issues with Senate Bill 5599
The main legal issue in question with Senate Bill 5599 is whether a state licensed agency such as a school or a homeless shelter can hide or kidnap a child who has ran away from their parents in order to allow “gender affirming treatment” which is treatment likely to permanently mutilate the child (and greatly increase the child’s risk of drug abuse, cancer and early death) without the parents knowledge or permission. The law covering this issue is RCW 13.32A.082. Providing shelter to minor—Requirement to notify parent.
Historically, state agencies had to notify parents where their child was within three days - except when there was a “compelling reason” not to notify the parents such as in cases of parental abuse of the child. In 2023, Senate Bill 5599 amended RCW 13.32A.082 to add a second compelling reason to not notify the parent. The second reason is when the child is seeking “gender affirming treatment” as defined in RCW 74.09.675.
RCW 74.09.675 is a law that was passed in 2021 and prohibited health insurance companies from excluding gender affirming care such as breast implants in their health plans. There is nothing in this law requiring medical treatment to minors. https://app.leg.wa.gov/RCW/default.aspx?cite=74.09.675
Senate Bill 5599 stated that the reason this exception to Parental Notice must be added to RCW 13.32A.082 was that the “Trevor project has found that one in three (33%) of transgender youth report attempting suicide.”
https://app.leg.wa.gov/billsummary?BillNumber=5599&Year=2023&Initiative=false
The unstated implication was that adding this exception would help reduce the suicide rate of Transgender youth.
Why Senate Bill 5599 was based on false data
Apparently, no one in the Senate bothered to check whether the claim that “one in three (33%) of transgender youth report attempting suicide” was true. Had they done even basic research, they would have quickly released that the claim was utterly false.
What the Trevor project actually did was mis-state the findings of the 2021 Center for Disease Control’s Youth Risk Behavior Survey (YRBS) which surveyed students in grades 9 to 12 about their risky behaviors. https://www.cdc.gov/healthyyouth/data/yrbs/index.htm
This data set did not include Washington state students but did include 1,485 high school students in the Seattle School district. Note that in 2021, there were about 15,000 high school students in the Seattle School District so the result is for only 10% of the students. Also, it is highly likely that many students who took the survey did not provide accurate answers.
Ignoring these problems for the moment, the 2021 national survey found that 7% of high school students reported that they attempted suicide. This does not mean that 7% actually attempted suicide but merely that they indicated that on their form. The actual number while bad is not known but it is certainly much less than 7%. A more accurate estimate is reported suicide attempts that resulted in a doctor report which was 2%.
Starting in 2015, a question to ascertain sexual identity was added to the national YRBS. Here is a link to a summary of the results of this questionnaire: https://www.cdc.gov/healthyyouth/data/yrbs/pdf/trendsreport.pdf
The 2015 to 2017 survey found that 23% of Trans high school students reported attempting suicide versus 7% among all students. 2% of straight students; 7.5% of trans students; and 5.6% of not sure students had made a suicide attempt resulting in an injury, poisoning, or overdose that had to be treated by a doctor or nurse.
Dramatic Rise in Trans Students from 2017 to 2021
In our public schools, there appears to be an explosion of Trans identifying students. The 2017 CDC survey found that 87% of students were straight, 9% trans (including gay, lesbian and bisexual) and 4% were not sure. The 9% trans result was dramatically higher than historical studies which concluded that less than 1% of adults were trans. The 2021 National Survey found that only 74% were straight. 15% were trans and 9% answered Do not know.
In 2021, of the 1,485 Seattle School District high school students who completed the survey, 980 (66%) were straight , 294 (19%) were trans and 211 (14%) answered Do not know. In short, about one in five Seattle High School students now claim to be Trans and one in seven Seattle High School students do not know what they are.
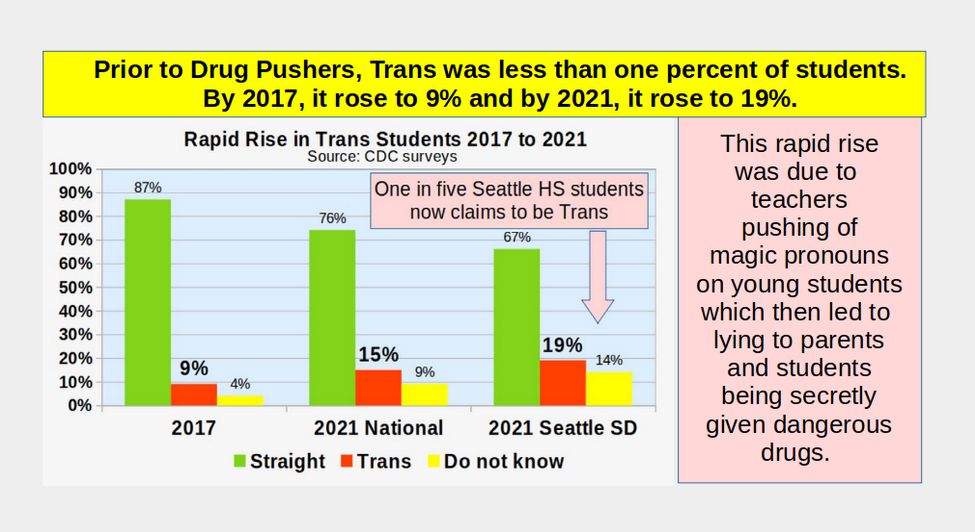
Among all Seattle High School students, 7% of all students reported having attempted suicide (the same as the national average). 2% reported the suicide attempt resulting in a doctor visit (the same as the national average). Among Seattle Trans students, 11% reported having attempted suicide with 4% resulting in a doctor visit.
https://nccd.cdc.gov/Youthonline/App/Results.aspx?LID=SE
In short, while the actual result of 11% of Trans students reporting to commit suicide – and 4% resulting in seeing a doctor - is still bad, it is much less than the 33% claimed in Senate Bill 5599 as the reason for hiding kids from their parents – and it is only slightly greater than the 7% national average.
More to the point is whether hiding gender-confused kids from their parents and injecting them with toxic drugs reduces the attempted suicide rate. We have already noted that among Trans adults who got the drugs, 42% reported attempting suicide versus 40% who did not get the toxic drugs.
Gallup Polls confirm the rise in Trans students is a social trend
Humans are herd animals. One of the key goals of growing up is to find a group where you can fit in and belong to. A danger of this need to belong is that teenagers are highly susceptible to joining cults. Here we define a cult as being a group that uses magical thinking to create a myth that promotes a radical lifestyle based on a series of lies. For example, cult members might believe that God is coming on a comet and they should all commit suicide when the comet passes by earth. Believing that a person can magically change their gender just by changing their pronouns and then taking a toxic mixture of drugs is only slightly less deadly.
As evidence that what is really happening is related to this generational cult formation, Gallup polls have found that the rise in the percentage of those who claim to be Trans is related to the thinking of their peers in their age group. As the chart below shows, each younger generation is about twice as likely as the generation that preceded it to identify as Trans. More than one in five Gen Z adults, ranging in age from 18 to 26 in 2023, identify as Trans, as do nearly one in 10 Millennials (aged 27 to 42). The percentage drops to less than 5% of Generation X, 2% of baby boomers and 1% of the Silent Generation.
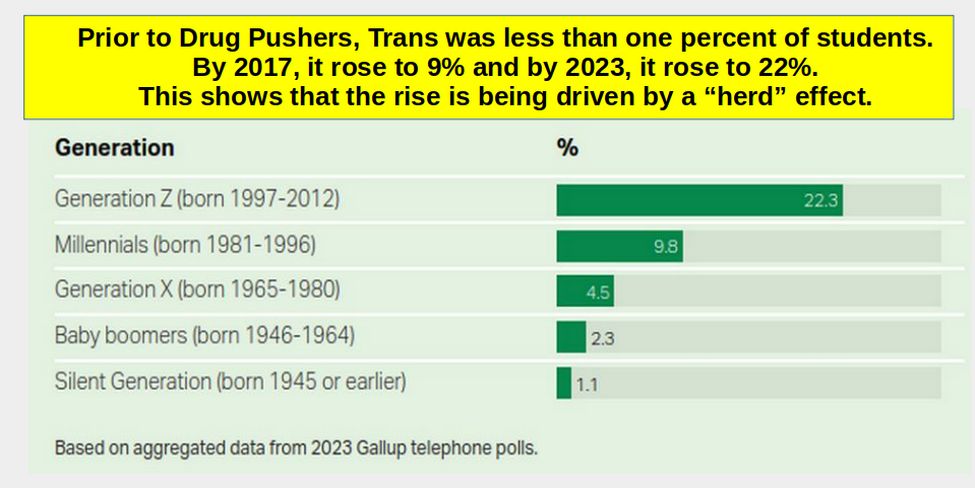
https://news.gallup.com/poll/611864/lgbtq-identification.aspx
We are thus witnessing the formation of a Trans Cult based on lies and propaganda being spread in our schools using the false claim that students need to be able to engage in magic thinking in order to reduce the risk of suicide. In addition, students need to be encouraged to lie to their parents because – well, because all cults tell their members to lie to their parents.
More Evidence that giving Minors access to drugs without their parents permission increases the suicide rate
In June 2022, the Heritage Foundation published a 25 page study confirming that states which passed laws such as Senate Bill 5599 which allowed minors access to danger drugs like puberty blockers and cross-sex hormones actually suffered an increase in suicides.
https://www.heritage.org/sites/default/files/2022-06/BG3712_0.pdf
Here are some quotes and graphs from this study:
In the past several years, the suicide rate among those ages 12 to 23 has become significantly higher in states that have a provision that allows minors to receive routine health care without parental consent than in states without such a provision. Before 2010, these two groups of states did not differ in their youth suicide rates. Starting in 2010, when puberty blockers and cross-sex hormones became widely available, elevated suicide rates in states where minors can more easily access those medical interventions became observable. Here are these states:
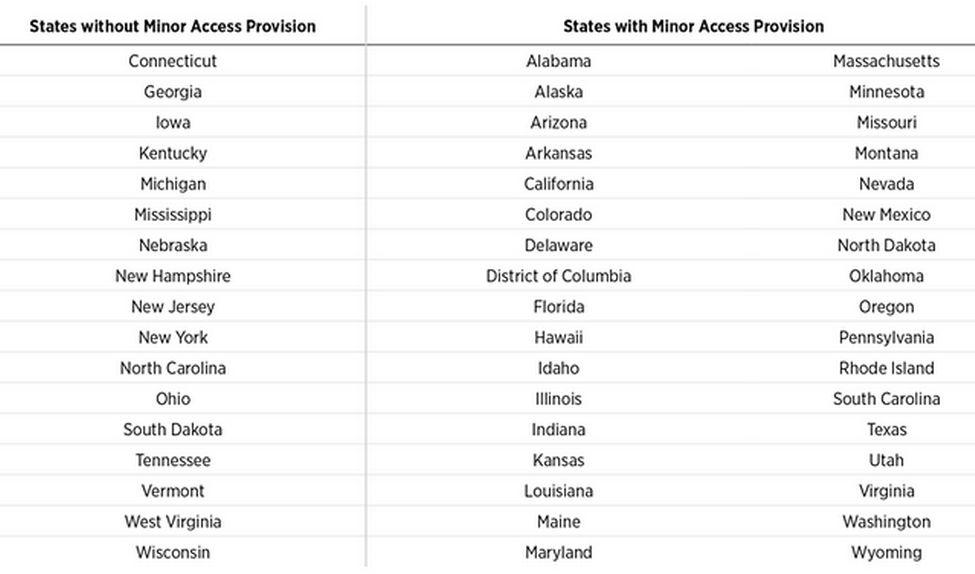
The following chart plots the difference in a three-year rolling average of suicide rates between states with minor access provisions and states with no such provision. Chart 2 plots the trend in this difference for those ages 12 to 23 who could have been affected by the policy when cross-sex medical interventions became available. For comparison, Chart 2 also shows the trend in this difference for a group ages 28 to 39, who could not have been affected by these policies, since the people in this group would have been at least 18 when puberty blockers and cross-sex hormones became available.
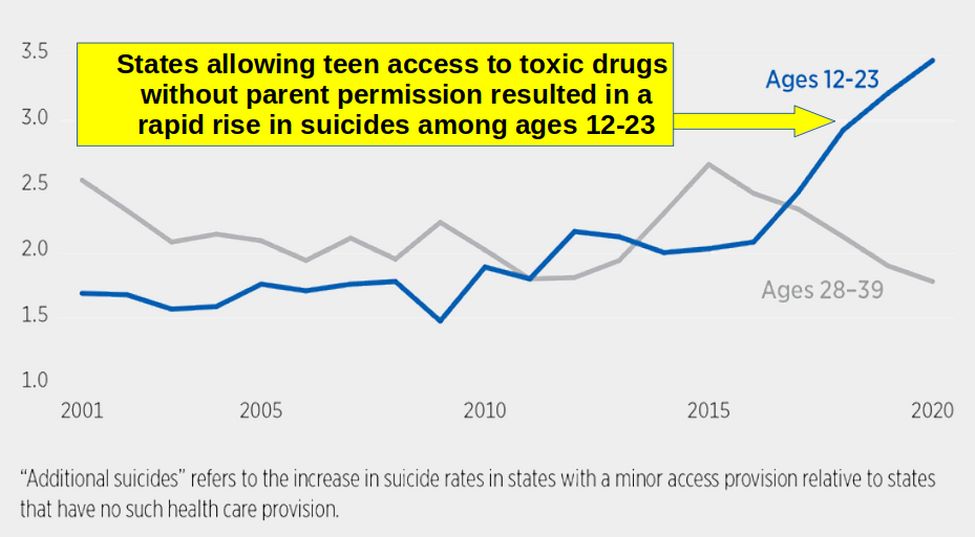
The suicide rates among those ages 12 to 23 (blue line) begin to spike in states that have provisions that allow minors to access health care without parental consent relative to states that have no such provision around 2016, after cross-sex medical interventions became more common.
By 2020, there are about 3.5 more suicides per 100,000 people ages 12 to 23 in states with easier access than in states without an access provision. There is no similar spike in suicide rates among those ages 28 to 39 (grey line) at that time.
Rather than being protective against suicide, this pattern indicates that easier access by minors to cross-sex medical interventions without parental consent is associated with higher risk of suicide.
States with a provision always had somewhat higher suicide rates than the states with no provision. To isolate the effect of this provision on youth suicide rates, it is better to control statistically for the youth suicide rate in each state at baseline as well as the suicide rate in each state in each year among the older and unaffected age group. Making these adjustments and plotting three-year rolling averages yields the trend pictured in Chart 3.
In 2015, the estimated increase in suicide rates in states with easier access accelerates. By 2020, there are about 1.6 more suicides per 100,000 people ages 12 to 23 in states that have a policy allowing minors to access health care without parental consent than in states without such a policy.
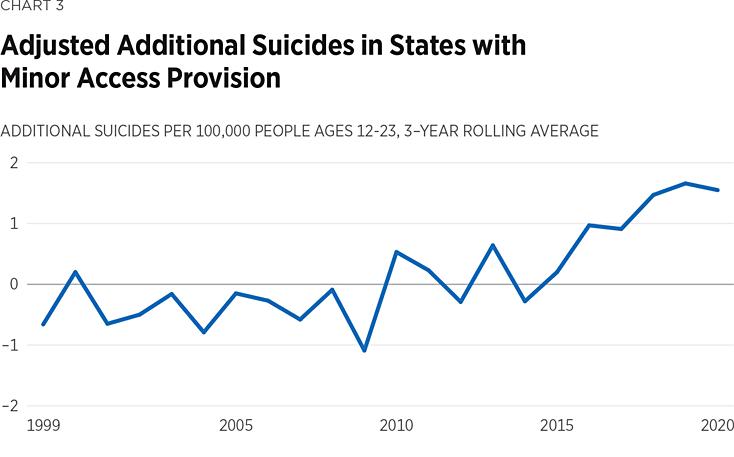
The results presented above provide strong evidence for that suicides among young people have increased significantly since 2010 in states that have a policy allowing minors to access routine health care without parental consent. That increase in suicide rates accelerated around 2016. Rather than lowering the suicide rate, Senate Bill 5599 is likely to increase it.
12 Backlash against SB 5599 led to the Parents Rights Initiative
As a consequence, on June 15, 2023, a group called Let’s Go Washington filed a Parents Rights Initiative (#I-2081) and began collecting signatures. The Initiative requires that parents be kept informed about materials their children are taught in K-12 classrooms and information about medical services public schools provide to their children. On December 12, 2023, the Initiative sponsors turned in 423,399 signatures which was 100,000 more than required.
On February 28, 2024, a joint House and Senate hearing was held on the Parents Rights Initiative. A total of 158 people signed in to testify and 6,477 provided online comments. As with the public comments previous year, over 98% of all comments were in favor of Parents Rights. Combining the two sets of comments, there were more than 11,000 comments in favor of parents rights and opposed to gender transitioning children without the consent or knowledge of their parents. Among those testifying “other” a representative of OSPI agreed that the Parents Rights Initiative did not violate any state or federal law and did not violate either the state or federal constitution. https://lawfilesext.leg.wa.gov/biennium/2023-24/Pdf/Bill%20Reports/Senate/I2081%20SIB%20EDU%20TA%2024.pdf
Also, no member of the House or Senate claimed that the Parents Rights Initiative might violate a state or federal law or the state or federal constitution. https://app.leg.wa.gov/billsummary?BillNumber=2081&year=2023&initiative=True
Here are a few of the Parents Rights Initiative Pro comments:
“I speak to you as the mother of a child who had a plan for suicide down on paper. Neither her counselor, her teacher, or her administrator told her father and I that she intended to kill herself. We saved our daughter, not the school system.”
The Legislature recently passed laws, including Senate Bill 5599, which eroded parents' rights and endangered children. The initiative will put control back with families, where it belongs. The initiative codifies the rights of parents to raise children without government interference. “
“Families are always a child's first teacher. Engaged parents raise happy and healthy kids. Studies show that when parents are involved and engaged, there is a significant impact on academic success. Schools should reduce barriers to parent and family participation to improve connection, collaboration, and transparency.
There have been numerous examples of teachers talking about sexuality and pronouns, and parents are not given the opportunity to opt their children out of this curriculum even when it goes against their religious and personal beliefs and family core values. The Parents Rights initiative helps assure parents that their rights and responsibilities for their child's well-being does not end at the schoolhouse door.
When an adult tells a child that they will keep secrets from their parents, it is a red flag. Parental rights are being infringed upon and parental preferences have been ignored. Parents are not being allowed to opt out of a curriculum that runs against their beliefs and values. It is important for school districts to listen to the concerns of students, families, staff, and communities.
On March 4, 2024, the Parents Rights Initiative passed in the House 82 to 15 and in the Senate 49 to 0. Crucially, not a single Representative or Senator claimed that the Parents Rights Initiative violated any current law or constitutional provision.
However, just because Senators voted for the bill does not mean they are in favor of Parents Rights. Instead, more than one legislator stated that if they had allowed the Parents Rights Initiative to go before the voters, they would not be able to amend it for TWO YEARS. By voting in favor of the Parents Rights Initiative this year, they can vote to “fix” (repeal or destroy) the Parents Rights Initiative as soon as next year!
13 May 2024 Legal Challenge to the Parents Rights Initiative
On May 6, 2024, the ACLU sent a letter to Washington State Attorney General Bob Ferguson demanding that his office investigate possible constitutional violations arising from the Parents Rights Initiative. On May 13, 2024, the Attorney General office declined to initiate legal proceedings. It is important to understand that if the Attorney General felt that the Parents Rights Initiative was against our State Constitution, he would be required as a matter of law to issue a statement saying this.
On May 23, 2024 the ACLU filed a 34 page lawsuit to prevent the Parents Rights Initiative from taking effect on June 6, 2024 because they claim that the initiative “contradicts existing federal and state laws… and the Washington state constitution.” The ACLU also claims that the initiative “misled state lawmakers and the public.” https://www.aclu-wa.org/docs/complaint-legal-counsel-youth-and-children-et-al-v-state-washington
The ACLU lawsuit asked King County Superior Court for a temporary restraining order, which would have prevented the initiative from taking effect on June 6 2024. However, the Court denied the motion. On June 21, the Court will consider a preliminary injunction. However, the ACLU case is so weak, it seems unlikely that the court will grant an injunction against an Initiative approved by a half million parents and passed in the Senate by a vote of 49 to zero.
14 State Superintendent Reykdal blocks Parents Rights Initiative
On June 5, 2024, Washington State Superintendent Chris Reykdal, issued a shocking last minute press release in which he advised school districts to ignore the Parents Rights Initiative. Contrary to OSPI testimony in February 2024, Reykdal now claims that certain provisions of the Parents Rights Initiative are in conflict with unspecified state and federal laws.
This is likely the first time in our state history that any state officer has asked school districts to ignore any state law. It is likely that Reykdal has no authority to advise school districts to ignore state law. It is also likely that Reykdal violated his Oath of Office in making this statement. While judges have the authority to put a law on hold while they review it, no one in the Executive Branch of state government has the authority to violate a law – even if it is a law that they do not personally agree with.
Washington Policy Center’s Liv Finne stated: “Superintendent Reykdal has crowned himself Supreme Ruler of Education Policy in Washington State. Above the people, the legislature and now the courts.”
Here is a link to Reykdal’s statement so you can read it yourself: https://ospi.k12.wa.us/about-ospi/news-center/news-releases-and-stories/washingtons-public-schools-will-continue-protect-student-privacy-and-safety
Why did Reykdal Block the Parents Rights Initiative?
One of the key provisions of the Parents Rights Initiative is that school districts would be required to tell parents about children who were being given gender transition treatments without the parents consent. Due to SB 5599, this disgusting form of extreme child abuse has been occurring in Middle Schools and High Schools in Seattle since July 2023. The services offered for children as young as 10 years old include “gender-altering medications (estrogen, androgen blockers, testosterone, etc.) and injection techniques,” “hormone therapy” and “referrals for gender surgeries.”
https://defendinged.org/incidents/seattle-public-schools-school-based-health-centers-offer-middle-and-high-school-students-access-to-gender-affirming-care-that-includes-hormone-therapy-and-referrals-for-surgeries/
Seattle Public Schools’ “Gender-Inclusive Schools: Transgender and Gender-Expansive Student Rights and Supports” (Policy 3211) states that “staff should not disclose a student’s transgender status to others unless (1) legally required to do so or (2) the student has authorized disclosure.” When “contacting the parents/guardians of a transgender student and it is unclear whether the student asserts the same gender identity at home, it is best practice to avoid using gender pronouns.”
Because the above Seattle School District policy is to actively hide the status of children from their parents, it is currently not known how many children in the Seattle School district are being subjected to gender mutilation without the knowledge or consent of their parents. But had Reykdal not issued his last minute block of the Parents Rights Initiative, at least some of these gender mutilation cases might have been exposed. Thus, the purpose of Reykdal’s statement was to give the Seattle School District an excuse to continue to keep this crime hidden from parents.

15 Federal Health Centers put in schools to avoid parental notice
To understand how this money making scam is run, we need to review federal and state medical privacy laws. The goal of the scam is to keep the gender mutilation brainwashing and treatment of the child hidden from parents as long as possible. This secrecy can be difficult in a school setting because federal FERPA laws require that “educational records” be shared with the parents.
These educational records include all records generated by any school employees – including school nurses. To get around the FERPA problem, the drug-controlled medical industry has created Federally qualified health centers (FQHCs) funded under Section 330 of the Public Health Service Act, 42 U.S.C. §§ 254b. These FQHCs are then placed in schools and made available to all students in the school district – even students who do not attend the school that the FQHC is located in. Health records created by employees working in a school setting such as a school-based health center but employed by a health entity are covered by HIPAA privacy laws, not FERPA privacy laws. Normally, under HIPAA, parents still need to be notified because normally under HIPAA, parents are assumed to “represent” the child and must give permission before treatment.
However, HIPAA has a sneaky loophole which is not present in FERPA. HIPAA rules can be over-ridden by State Medical Privacy Rules! States can and do allow some minors to grant permission for some medical procedures without telling their parents. For example, in Washington State, we have “Minor Consent Laws.” Minor consent laws allow minors to consent for their own care in specific situations and for specific services. Minors can consent for contraception, pregnancy care, and abortion. Minors may also access emergency contraception without parental consent. However, as of March 2019, our state’s minor consent laws do not explicitly provide for minors to consent for transgender services.
https://nahic.ucsf.edu/wp-content/uploads/2019/01/Washington-AYAH-Confidentiality-Guide_FInal.pdf
Federal health centers in Washington Schools
The number of School Based Health Centers (SBHCs) in Washington State has more than doubled from under 30 in 2019 to more than 70 in 2024. SBHCs are now located in more than 30 school districts in Washington state. A table of these SBHCs is at the end of this section. The expansion was related to millions of dollars in new state and federal funds which increased greatly in 2021 and again in 2022.
SBHCs require the approval of your local school board which must provide space for the SBHC inside of a local school. Essentially, the school board approves and pays for converting a portion of a school building into a non-school space so a third party organization can operate an independent business on the school premises in order to bypass state and federal parental notification laws.
The state and federal parental notification laws are bypassed because the employees of the SBHC are not technically employees of the school district. Instead, these SBHCs are often run by Federally Qualified Community Health Centers (FQHC) which are partially funded by the federal government. Washington State now has 29 Federally Qualified Community Health Centers (FQHC).
The danger of SBHCs is that parents and students can be misled into thinking that the SBHC is a part of the school when it is in fact a separate business. Parents may not know that students can receive experimental and even dangerous gender mutilation drugs at an SBHC without their parents knowledge or consent.
Advocates of Gender Mutilation drugs (also called Gender Affirming Care) claim that giving kids gender drugs saves lives and reduces the suicide rate. In fact, giving kids gender drugs is known to cost lives and increase the suicide rate.
Advocates of SBHCs also claim that they increase attendance. However, while SBHCs have doubled since 2019, the chronic absentee rate in Washington state has risen from 15% of students to 30%.
Advocates of SBHCs also claim that they increase parent engagement. Instead, SBHC’s are specifically run to eliminate parental notice.
Advocates of SBHCs also claim that they lower health care costs. Instead, SBHCs have dramatically raised health care costs for minors as secretive and dangerous gender mutilation drugs can cost hundreds of thousands of dollars per child.
For example, two of the 29 FQHCs are Neighbor Care Health and Country Doctor. https://www.wacommunityhealth.org/community-health-centers-1
In Snohomish County, one that operates in two public schools is Community Health Center of Snohomish County. They are located at two high schools in the Edmonds School District.
https://www.chcsno.org/

Both clinics are operated by the Community Health Center of Snohomish County and funded by the Verdant Health Commission.
In Seattle, the School Based Health Clinics appear to be funded by Seattle tax payers.
https://www.seattle.gov/education/fepp-levy/school-based-health-centers
Here is a quote and image from their website:
“K-12 School Health investments provide students with increased access to medical and mental health care through School-Based Health Centers (SBHCs), school nursing, oral health care and health system enhancements. These strategies promote the early intervention, prevention, and treatment of … gender competency, and provide an accessible source of health care.

17,941 Students Served In SY 2021-22. As part of the City’s $4.5 million investment to increase student mental health supports in schools, the Seattle Department of Education and Early Learning (DEEL) is launching a funding process to expand services at up to three additional schools
Access to SBHCs is available for all Seattle Public Schools students regardless of the presence of an SBHC on their school campus. While services are universally accessible to all SPS students, outreach and referrals for services are focused on students with the greatest need such as … LGBTQ students.
DEEL partners with Public Health - Seattle & King County (PHSKC) to administer School-Based Health Centers. PHSKC's role includes managing SBHC contracts with healthcare providers, overseeing Request for Application processes, and providing direct services at three SBHCs within Seattle Public Schools (Cleveland, Ingraham, and Rainier Beach high schools).”
Here is a table of School Based Health Centers in Washington State (Seattle School Based Health Centers including 9 elementary schools, 8 middle schools and 14 high schools). Source: https://wasbha.org/sbhcs-in-washington-2/
|
County
|
School District
|
School
|
Healthcare Sponsor (FQHC)
|
|---|
|
Clallam
|
Port Angeles
|
Mobile clinic serving all schools
|
North Olympic Healthcare Network
|
|
Clark
|
Evergreen
|
Evergreen High School
|
Sea Mar Health Centers
|
|
Grant
|
Quincy
|
Quincy High School
|
Moses Lake Health Center
|
|
Grays Harbor
|
Elma
|
Elma Elementary School
|
Educational Service District 113
|
|
Jefferson
|
Chimacum
|
Chimacum High School
|
Jefferson County Public Health
|
|
Jefferson
|
Port Townsend
|
Port Townsend High School
|
Jefferson County Public Health
|
|
Jefferson
|
Quilcene
|
Quilcene K-12
|
Jefferson County Public Health
|
|
King
|
Bellevue
|
Highland Middle School
|
International Health Services
|
|
King
|
Federal Way
|
TAF@Saghalie>;
|
Healthpoint
|
|
King
|
Federal Way
|
Thomas Jefferson High School
|
Healthpoint
|
|
King
|
Renton
|
Renton High School
|
Healthpoint
|
|
King
|
Highline
|
Tyee High School
|
Healthpoint
|
|
King
|
Highline
|
Evergreen High School
|
Healthpoint
|
|
King
|
Seattle
|
Aki Kurose Middle School
|
Kaiser Permanente
|
|
King
|
Seattle
|
Bailey Gatzert Elementary School
|
Neighborcare Health
|
|
King
|
Seattle
|
Ballard High School
|
Swedish Medical Center
|
|
King
|
Seattle
|
Beacon Hill International School
|
Odessa Brown Children’s Clinic
|
|
King
|
Seattle
|
Chief Sealth High School
|
Neighborcare Health
|
|
King
|
Seattle
|
Cleveland High School
|
Public Health-Seattle & King County
|
|
King
|
Seattle
|
Dearborn Park Elementary School
|
Neighborcare Health
|
|
King
|
Seattle
|
Denny International Middle School
|
Public Health-Seattle & King County
|
|
King
|
Seattle
|
Franklin High School
|
Kaiser Permanente
|
|
King
|
Seattle
|
Garfield High School
|
Odessa Brown Children’s Clinic
|
|
King
|
Seattle
|
Highland Park Elementary School
|
Neighborcare Health
|
|
King
|
Seattle
|
Ingraham High School
|
Public Health-Seattle & King County
|
|
King
|
Seattle
|
Interagency Academy
|
Kaiser Permanente
|
|
King
|
Seattle
|
Lincoln High School
|
Neighborcare Health
|
|
King
|
Seattle
|
Lowell Elementary
|
Odessa Brown Children’s Clinic
|
|
King
|
Seattle
|
Madison Middle School
|
Neighborcare Health
|
|
King
|
Seattle
|
Meany Middle School
|
Country Doctor
|
|
King
|
Seattle
|
Mercer International Middle School
|
Neighborcare Health
|
|
King
|
Seattle
|
Nathan Hale High School
|
Kaiser Permanente
|
|
King
|
Seattle
|
Nova High School
|
Country Doctor
|
|
King
|
Seattle
|
Rainier Beach High School
|
Public Health-Seattle & King County
|
|
King
|
Seattle
|
Rising Star @ African American Academy
|
Neighborcare Health
|
|
King
|
Seattle
|
Robert Eagle Staff Middle School
|
Neighborcare Health
|
|
King
|
Seattle
|
Roosevelt High School
|
Neighborcare Health
|
|
King
|
Seattle
|
Roxhill Elementary School
|
Neighborcare Health
|
|
King
|
Seattle
|
Seattle World School
|
International Community Health Services
|
|
King
|
Seattle
|
Washington Middle School
|
Kaiser Permanente
|
|
King
|
Seattle
|
West Seattle Elementary School
|
Neighborcare Health
|
|
King
|
Seattle
|
West Seattle High School
|
Neighborcare Health
|
|
King
|
Auburn
|
Auburn Mountainview High School
|
Sea Mar Health Centers
|
|
King
|
Highline
|
Highline High School
|
Healthpoint
|
|
King
|
Vashon
|
Vashon High School, Chautauqua Elementary and McMurray Middle Schools
|
Neighborcare Health
|
|
Kitsap
|
Bremerton
|
Bremerton High School
|
Peninsula Health Services
|
|
Kitsap
|
Bremerton
|
Mountain View Middle School
|
Peninsula Health Services
|
|
Kitsap
|
Central Kitsap
|
Barker Creek Community School
|
Peninsula Health Services
|
|
Kitsap
|
Central Kitsap
|
Esquire Hills Elementary School
|
Peninsula Health Services
|
|
Kitsap
|
Central Kitsap
|
Fairview Junior High School
|
Peninsula Health Services
|
|
Kitsap
|
Central Kitsap
|
Olympic High School
|
Peninsula Health Services
|
|
Kitsap
|
North Kitsap
|
Kingston High School
|
Peninsula Health Services
|
|
Kitsap
|
South Kitsap
|
Discovery Alternative School
|
Peninsula Health Services
|
|
Kitsap
|
North Kitsap
|
Poulsbo Middle School
|
Peninsula Health Services
|
|
Kitsap
|
Central Kitsap
|
Central Kitsap High School
|
Peninsula Health Services
|
|
Kitsap
|
Central Kitsap
|
Klahowya Secondary
|
Peninsula Health Services
|
|
Mason
|
North Mason
|
North Mason High School, Hawkins Middle School and James Taylor High School
|
Peninsula Health Services
|
|
Pend Oreille
|
Newport
|
Newport High School
|
Newport Hospital and Health Services
|
|
Pend Oreille
|
Newport
|
Pend Oreille River School
|
Newport Hospital and Health Services
|
|
Pend Oreille
|
Newport
|
Sadie Halstead Middle School
|
Newport Hospital and Health Services
|
|
Pend Oreille
|
Newport
|
Stratton Elementary School
|
Newport Hospital and Health Services
|
|
Pierce
|
Bethel
|
Bethel Middle School, Bethel High School and Shining Mountain Elementary
|
Community Health Care
|
|
Pierce
|
Tacoma
|
Mt. Tahoma High School
|
MultiCare
|
|
Skagit
|
Sedro-Woolley
|
Sedro-Woolley High School
|
PeaceHealth
|
|
Snohomish
|
Edmonds
|
Meadowdale High School
|
Community Health of Snohomish County
|
|
Snohomish
|
Edmonds
|
Mountlake Terrace HS
|
Community Health of Snohomish County
|
|
Spokane
|
Mead
|
Shiloh Hills Elementary School
|
CHAS Health
|
|
Spokane
|
Spokane
|
Excelsior Holistic School
|
Excelsior Family Medicine
|
|
Spokane
|
Spokane
|
Lumen High School
|
Excelsior Family Medicine
|
|
Spokane
|
Spokane
|
Rogers High School
|
CHAS Health
|
|
Walla Walla
|
Walla Walla
|
Lincoln High School
|
The Health Center
|
|
Walla Walla
|
Walla Walla
|
Pioneer Middle School
|
The Health Center
|
|
Walla Walla
|
Walla Walla
|
Walla Walla High School
|
The Health Center
|
|
Whatcom
|
Lummi Nation
|
Lummi Nation School
|
Lummi Tribal Health Clinic
|
Each of the above agencies are ignoring the science on how gender drugs are neither safe or effective.
16 Washington laws promoting Gender Mutilation of Minors
Four recent laws promoting gender mutilation of minors that have led to the rapid expansion of SBHCs in Washington State include:
Senate Bill 5689 which was passed in 2019. While this bill claimed to be about reducing bullying in schools, it was instead a bill to promote radical and harmful gender ideology in schools. Here is a quote from this bill:
“The Washington state school directors' association must collaborate with the office of the superintendent of public instruction to develop and update a model transgender student policy and procedure… under RCW 28A.642.020 to eliminate discrimination in Washington public schools on the basis of gender identity.”
Apparently, the above language requires allowing boys in girls bathrooms, girls locker rooms and girls sports. With the gender-inclusive school policies, state schools are teaching young, easily manipulated children radical gender ideology from the day they enter kindergarten. Students are being taught that it’s okay to hide things from their parents. They’re being taught lies about their identity. It’s not optional, it’s state law. Who could have known?
House Bill 1225 passed in 2021. Concerning school-based health centers. Ironically, this bill has not a single word about providing gender mutilation drugs to minors. Just that these SBHCs will be coordinated by the Washington State Department of Health – the same people that brought us the ridiculous school closures, business closures, mask mandates and shot mandates as well as the wildly inaccurate PCR tests for Covid-19.
Here are some of the comments from those opposed to this bill:
“School districts should maintain the discretion to decide whether to establish SBHCs. This bill takes away local control and gives the Department of Health (DOH) too much decision-making authority. It is unclear why nonprofit organizations need to be involved in establishing or supporting SBHCs. The DOH's process for awarding grants should take place in a subcommittee where there will be full transparency and opportunities for public comments. School districts should have final decision-making authority and be able to turn down grant funding without any ramifications.”
“Families should be in charge of their children's health care. School-based health centers cannot take the place of existing providers that families already trust to administer care to their children. School-based health centers take advantage of the lack of parental oversight and administer services without parental involvement or knowledge, especially with regard to students that are 13 years of age or older who can consent to treatment without a parent’s consent or knowledge. “
Senate Bill 5599 passed in 2023 removed parental notice or consent for gender mutilation drugs being given to minors and allows the state to not notify parents if the child thinks their parents may not be “affirming” of their choice to take gender mutilation drugs.
House Bill 2331 passed in 2024 eliminating local control of school curriculum. This bill requires the punishment of any school district that dares to defy the radical agenda of Reykdal and the legislature by banning either the Gender Mutilation curriculum or the Racial Shaming curriculum. Here is a quote: “The SPI (Reykdal) has the power to enforce state laws prohibiting discrimination by instituting corrective action, terminating the offending program, placing the school district on probation, or withholding state funds.”
“Any person aggrieved by a violation of nondiscrimination provisions, or aggrieved by the violation of any rule or guideline adopted in accordance with the nondiscrimination provisions, has a right of action in superior court for civil damages and such equitable relief as the court determines.”
“A school district board of directors (school board) may not refuse to approve, or prohibit the use of, any textbook, instructional material, supplemental instructional material, or other curriculum for student instruction on the basis that it relates to or includes the study of the role and contributions of any individual or group that is part of a protected class as established in public school nondiscrimination provision.”
Here are some of the comments from those opposed to this bill:
The idea of defunding schools up to 100 percent for unclear violations is objectionable. This bill may lead to further erosion of public school enrollment. The only way to ensure that the needs of students and communities are met is through locally determined decisions. School directors should focus on making sure that students can read rather than promoting radical ideologies.
Some books that have been widely pushed contained inappropriate content, including content of a sexual nature. Parents are not trying to ban books, they are trying to keep them away from minors.
Forty thousand families have left failing Washington schools. If policymakers keep up this politicized agenda, every school levy will fail. This bill is government overreach. No one person, even a school librarian, has the right to expose students to pornography. Efforts to insert pornography into school libraries are wrong. Children should be protected from inappropriate materials.
17 US Supreme Court ruling on Parents Rights
In 1925, the US Supreme Court unanimously struck down an Oregon law requiring children to attend public schools because the law interfered with the right of parents to select a private or parochial school for their children. Parents have a fundamental constitutional right to rear their children, including the right to determine who shall educate and socialize them:
“The fundamental theory of liberty upon which all governments in this Union repose excludes any general power of the State to standardize its children by forcing them to accept instruction from public teachers only. The child is not the mere creature of the State; those who nurture him and direct his destiny have the right, coupled with the high duty, to recognize and prepare him for additional obligations.” Pierce v. Society of Sisters, 268 U.S. 510 (1925)
“It is cardinal with us that the custody, care and nurture of the child reside first in the parents, whose primary function and freedom include preparation for obligations the state can neither supply nor hinder. . . . It is in recognition of this that these decisions have respected the private realm of family life which the state cannot enter.” Prince v. Commonwealth of Massachusetts, 321 U.S. 158 (1944)
“The right of the family to remain together without the coercive interference of the awesome power of the state . . .encompasses the reciprocal rights of both parent and child.” The court explained that children have the constitutional right to avoid dislocation from the emotional attachments that derive from the intimacy of daily association with the parent.” Duchesne v. Sugarman, 566 F.2d 817, 825 (2d Cir. 1977).
“In a long line of cases, we have held that, in addition to the specific freedoms protected by the Bill of Rights, the "liberty" specially protected by the Due Process Clause includes the rights . . . to direct the education and upbringing of one's children.” - Washington v. Glucksburg, 521 U.S. 702 (1997)
“The liberty interest at issue in this case-the interest of parents in the care, custody, and control of their children-is perhaps the oldest of the fundamental liberty interests recognized by this Court. In light of this extensive precedent, it cannot now be doubted that the Due Process Clause of the Fourteenth Amendment protects the fundamental right of parents to make decisions concerning the care, custody, and control of their children… The Due Process Clause does not permit a State to infringe on the fundamental right of parents to make child rearing decisions simply because a state judge believes a 'better' decision could be made.” - Troxel v. Granville, 530 U.S. 57 (2000)
In response to a public school district’s subjection of children to inappropriate and sexually explicit content, the United States House of Representatives affirmed that “the fundamental right of parents to direct the education of their children is firmly grounded in the Nation’s Constitution and traditions.” House Resolution 547 (November 16, 2005)
While 25 states have passed bans on any gender mutilation of minors, on May 22, 2024, the California State Senate passed a bill prohibiting schools from notifying parents of a child’s pronoun change. https://apnews.com/article/california-gender-pronouns-schools-transgender-ccd2c81345428c3c0a5d9e41565598d2
It is likely that if a Democrat majority is elected in 2024, they will pass a similar law in Washington state in 2025. It is also likely that schools will never notify parents as long as Reykdal is State Superintendent.
This is why we have started the Washington Parents Network – to inform parents about the crimes being committed against their kids – and to organize parents into electing representatives who are more aware of the importance of protecting children from gender mutilation and protecting a child’s right to a positive relationship with their parents.
18 Exposing WPATH Crimes against children
On March 5, Mia Hughes published a 241 page report exposing crimes against children committed by the leaders of the World Professional Association for Transgender Health also known as WPATH. This is a group of Trans advocates responsible for the experimental gender mutilation processes that thousands of children in the US are currently being subjected to. You can download the WPATH report at this link:
https://static1.squarespace.com/static/56a45d683b0be33df885def6/t/6602fa875978a01601858171/1711471262073/WPATH+Report+and+Files111.pdf
The evidence in this report comes directly from internal WPATH emails and other internal documents – all of which confirm that WPATH is neither a scientific nor medical organization. The medical abuse of minors, known as “gender-affirming care,” are unethical medical experiments. WPATH leaders advocate for the destruction of healthy reproductive systems, the amputation of healthy breasts, and the surgical removal of healthy genitals as the first and only line of treatment for minors with gender dysphoria.
WPATH go its start in 2007 – immediately appointing themselves as the world’s leading international authority on gender medicine. In 2012, they published Standard of Care (SOC) 7 which recommended experimental puberty blockers and framed being transgender as a normal, healthy, variation of human existence. In 2022, they published SOC 8 which removed almost all lower age requirements. This attack against children led to the formation of an ANTI-WPATH group called Beyond Wpath in 2022. Here is a link to their website: https://beyondwpath.org/
Beyond WPATH has 2755 signers who are all opposed to WPATH. Here is a quote from their website: As mental health professionals, public health scientists, and allied organizations and individuals, we have grave concerns about the damaging physical and mental health impacts of the current Standards of Care released by WPATH (the World Professional Association for Transgender Health). We hold that WPATH has discredited itself. We are signing this Declaration to highlight our grave concerns about WPATH’s Standards of Care, and to encourage parents, schools, psychotherapists, and other health care professionals to utilize the wealth of alternative resources that are now widely available.
The organizations, physicians, research scientists, mental health professionals, and other signatories to this Statement stand together in supporting alternatives to WPATH’s deeply flawed Standards of Care. We align with the most up-to-date science-based guidelines from those countries which have already evaluated and rejected the affirmative approach. We believe health care professionals serving the needs of gender-questioning youth can honor and respect their rights without subscribing to a flawed ideological document marred by ethical failures and factual errors.
We hold that the authoritative status of WPATH’s Standards of Care is fatally undermined by the following errors and ethical failures: The Standards specifically promote the affirmative care model, continuing to endorse widespread medical treatments (drugs and surgery) for trans-identified youth despite rising scientific skepticism that has led Sweden, Finland, France, and the United Kingdom to retreat from that approach. WPATH endorses early medicalization as fundamental while these other countries now promote psychosocial support as the first line of treatment. For these and other reasons, we believe WPATH can no longer be viewed as a trustworthy source of clinical guidance in this field.
The WPATH Files contain abundant evidence that the world-leading transgender health group does not respect the well-established scientific process – as is summarized in the following report:
January 2023 Abbruzzese et al “The Myth of “Reliable Research” in Pediatric Gender Medicine: A Critical Evaluation of the Dutch Studies—and Research That Has Followed.”
https://doi.org/10.1080/0092623x.2022.2150346
The WPATH Files contain abundant evidence demonstrating just how little is known about the puberty blocking and sex hormone drugs and their long-term effects. For example, in the first long term study of minors using puberty suppressors and sex hormones in 2022 found that 27% of the young people who had undergone early puberty suppression followed by sex hormones and surgical removal of the testes or ovaries, at an average age of 32, regretted sacrificing their fertility.
Following systematic reviews of evidence, three European countries—Sweden, Finland and England—have adopted new and much more cautious treatment guidelines for gender dysphoric youth, which prioritize noninvasive psychosocial interventions.
There is no argument that the Dutch experience, and in particular two Dutch studies—de Vries et al. (Citation2011), and de Vries et al. (Citation2014)—forms the foundation of the practice of youth gender transition. It is evident when examining prevailing treatment guidelines.
What the two Dutch studies failed to show, however, is that these physical changes resulted in meaningful psychological improvements significant enough to justify the adverse effects of the treatment—including the certainty of sterility.
Besides the lack of a control group and a small final sample of 55 cases, with key outcomes available for as few as 32 individuals, there are three major areas of concern that render these studies unfit for clinical or policy decision-making.
The Dutch studies did not evaluate physical health outcomes of “gender-affirmative” treatments. Even without setting out to assess the risks, the Dutch research inadvertently revealed that the rate of short-term morbidity and mortality associated with “gender-affirming” interventions is as high as 6%-7%.
The actual outcome is likely to be much worse because the Dutch studies “cherry picked” from an original sample of 196 referred cases by only including the 55 cases with the most desirable outcomes. Even with this, adverse outcomes included severe diabetes, obesity and one death.
Several studies since have confirmed likely adverse health effects of hormonal interventions. Research suggests heightened insulin resistance (Nokoff et al. 2021), elevated blood pressure, elevated triglycerides, and impaired liver function (Olson-Kennedy, Okonta, et al., 2018). Cross-sex hormone administration places adolescents in the medical category of early life indicators of future cardiovascular disease (Jacobs et al., 2022).
At least two studies confirm that psychological interventions absent any medical interventions. are associated with improvements in two of the outcome domains—gender dysphoria (van de Grift et al., 2017) https://pubmed.ncbi.nlm.nih.gov/28319558/
and global function (Costa et al., 2015) https://pubmed.ncbi.nlm.nih.gov/26556015/
Around 2015 the presentation of pediatric gender dysphoria in the Western world sharply shifted, from childhood-onset that skewed toward males, to adolescent-onset with a preponderance of females with mental health problems. Finnish researchers saw a new pattern of “severe psychopathology preceding onset of gender dysphoria,” with 75% already in treatment for other psychiatric issues when their gender dysphoria emerged. Between 2009 and 2016, the number of gender dysphoric females increased more than 70 times. In the US, over 70% of gender dysphoric youth have also been diagnosed with ADHD and other mental health problems before their diagnosis of gender dysphoria (Becerra-Culqui et al., 2018).
Subsequent detransitioner research confirmed that patients reported “that their gender dysphoria began during or after puberty and that mental health issues, trauma, peers, social media, online communities, and difficulty accepting themselves as lesbian, gay, or bisexual were related to their gender dysphoria and desire to transition” (Littman, 2021, p. 15)
The few attempts at long-term follow-up for adults who have undergone sex-trait modification interventions do not show positive outcomes, with individuals showing social difficulties and a significantly elevated rate of completed suicides and mental health issues.
Also, a 2018 study conducted by Kaiser Permanente found that natal males on estrogen had a 5.2% risk of a blood clot in the lungs or legs, a heart attack, or a stroke within 4 years after initiating estrogen (but the increased risk begins as early as one year), and the risks rise the longer a trans-identified natal male takes estrogen. Getahun, D., et al. (2018). Cross-sex Hormones and Acute Cardiovascular Events in Transgender Persons. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6636681/pdf/nihms-1030323.pdf
Given the lack of scientific literature to indicate that cross-sex hormone therapy is safe and effective, as well as the number of known negative side effects and the possible serious negative outcomes, it is unethical for WPATH to advocate for minors and the severely mentally ill to bypass psychotherapy and have immediate access to these powerful drugs.
The deliberate avoidance of the term “experimental” is due to the fact that experimental medicine is not covered by health insurance, and one of the primary objectives of WPATH’s SOC8 is to secure insurance coverage.
Many detransitioners feel intense anger and grief regarding the irreversible changes wrought by gender-affirming care. They mourn the loss of their body parts and the experiences, such as bearing children or breastfeeding, that have been taken from them.
Changing names and pronouns is often portrayed as a harmless, non-medical step to alleviate a child’s distress. It is sold to parents as completely reversible at any time, but all available evidence suggests the contrary - social transition serves to lock in the transgender identity and leads to puberty blockers. Almost every adolescent who commences puberty blockers proceeded to cross-sex hormones.
Blocking puberty, therefore, means blocking the natural cure to gender dysphoria robbing children of the same developmental process that would almost certainly have enabled them to overcome their dysphoria naturally.
The Transition-or-Suicide Myth makes the false promise that these experimental interventions will eliminate the risk of suicide for the young person when no evidence exists to support such a claim. A Swedish study of 324 individuals who had undergone genital surgery between 1973 and 2003 revealed rates of completed suicide post-surgical transition to be greatly elevated over the general population, with trans-identified natal females 40 times more likely to die by suicide and trans-identified natal males 19 times more likely.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3043071/pdf/pone.0016885.pdf
19 Inside the Gender Mutilation Scam Industry
On June 18, 2024, a former gender mutilation nurse named Vanessa Sivadge exposed the degree of fraud that occurs in the disgusting gender mutilation business. According to Venessa, doctors at Texas Children’s Hospital falsified medical records and broke the law to keep practicing “gender-affirming care”. They also committed Medicaid fraud to secure funds for the hospital’s child sex-change program. Here is a link to the article: https://www.city-journal.org/article/the-murky-business-of-transgender-medicine
Here are quotes from the article:
“Beginning in 2021, Sivadge saw a dramatic rise in the number of “transgender children” treated at the hospital. These patients struggled with various problems: depression, anxiety, addiction, suicide attempts, physical abuse, and discomfort with puberty. But rather than deal with these underlying psychological conditions, doctors at the hospital would diagnose them with “gender dysphoria” and assign them to “gender-affirming care. The practice made Sivadge recoil. “In the cardiac clinic, we were taking sick kids and making them better. In the transgender clinic, it was the opposite. We were harming these kids.”
Then, in 2022, she breathed a sigh of relief. Under pressure from the state attorney general, Ken Paxton, Texas Children’s CEO Mark Wallace said that he was shutting down the child gender clinic. But it wasn’t true. Mere days later, it had secretly reopened for business. And business was booming. Doctors were managing dozens of pediatric sex-change cases, performing surgeries, blocking puberty, and implanting hormone devices.
In Sivadge’s view, Roberts and other providers were manipulating patients into accepting “gender-affirming care.” When parents objected, the doctors bulldozed them, she claims. Some families, she believed, feared that the hospital would call Child Protective Services if they dissented.
Texas Children’s Hospital continued its sex-change program but focused now on patients who had reached the legal age of 18. Sivadge saw the same terrible medical regimen being prescribed for these young adults: testosterone for girls, estrogen for boys, and referrals for specialty services. While Roberts and Paul had stopped providing sex-change procedures for minors, the gender clinic still overflowed with “transgender” teens.
Sivadge’s duties as a nurse included providing medication refills and working with doctors to provide parents with information about treatment plans. She worked with patients’ charts and saw their complex psychological diagnoses and the treatments administered by the doctors.
Then Sivadge noticed discrepancies in the paperwork. She followed some of the medical charts for these patients and came to believe that doctors might be violating the law. As Sivadge learned, Texas law forbade hospitals from billing Medicaid for transgender procedures. The Texas Medicaid Provider Procedures Manual has long stated that “sex change operations” are “not benefits of Texas Medicaid.” In 2021, Texas Medicaid officials told the Kaiser Family Foundation that this prohibition was not limited to genital surgeries but “explicitly excludes coverage of all gender affirming health services.” In Texas, Medicaid and the Children’s Health Insurance Program already don’t cover transition-related surgeries and prescription drugs like hormone therapies and puberty blockers.
At Texas Children’s, as she was treating patients, Sivadge carefully scrutinized the treatments related to an alarming number of “transgender” teenagers, who, she came to believe, were unlawfully billing the state Medicaid program. One patient, whom we’ll call Patient A, began treatment at Texas Children’s in 2022, at the age of 16. Patient A is a biological female who identified as “non-binary” and whose records claimed that she was “male.” This patient began treatment with a prescription for testosterone as part of the patient’s “gender-affirming” medical regimen. During treatment, Roberts explained to Patient A the effects of testosterone, including masculinization and the suppression of fertility, and had her continue with testosterone injections.
Another patient, whom we’ll call Patient B, began care at Texas Children’s in 2022, also at the age of 16. Patient B is a biological male who identified as a female and whose records indicated the transgender identity, “female.” He arrived at the gender clinic under the care of Paul, already having begun a prescription of a testosterone blocker and estrogen, which served as a sex-change hormone. Patient B had increased the size of his breasts but was frustrated by the persistence of facial hair. Paul discussed changing the testosterone blocker and increasing the dose of estrogen in order to make progress with feminization. Patient B told Paul that he wanted his breasts to be larger. Paul adjusted Patient B’s estrogen prescription and discussed the possibility of breast implants.
Sivadge noticed another critical piece of information: Patient A and Patient B, like several other “transgender” patients, were enrolled in Texas Children’s Health Plan STAR, a “no-cost Medicaid managed care plan.” Despite the law, which prohibited billing Medicaid for “gender-affirming care,” it appears that this was a standard practice at Texas Children’s Hospital. As Roberts himself admitted in a 2023 affidavit related to the lawsuit against SB 14, he had several patients in his transgender medicine program “who receive their health coverage through Medicaid.”
According to a legal expert with deep knowledge of Texas Medicaid law, the essential facts are as follows: Patients A and B had coverage through Texas Children’s Plan STAR; the doctors explicitly treated them for the purpose of “gender-affirming care”; and the standard practice would be for the hospital to submit this care for reimbursement through the state Medicaid program. “Based on the facts we have, the only reasonable conclusion is that Texas Children’s Hospital was using Texas Medicaid funds to pay for ‘gender-affirming care,’ contrary to Texas law,” said the legal expert.
For Sivadge, there was no doubt about what was happening. “The largest children’s hospital in the country is illegally billing Medicaid for transgender procedures,” she said. “It is evident that the hospital continues to believe it is above the law not just by concealing the existence of their transgender medicine program from the public, but by stealing from the federal government.”
Sivadge now feels regret. “I was told to do something I knew was wrong. It made me sick that the lie called ‘gender-affirming care’ was being sold to parents and children and creating hugely lucrative profits in secret—and I was part of it.”
Sivadge is not the only one feeling regret. Doctors, families, and political leaders are all starting to question the folly of child sex-change programs. The sense is growing that the public was sold a bill of goods—and that children are being put in grave danger.
20 Rapid Onset Gender Dysphoria
Since 2018, hundreds of parents have claimed that their previously normal children, who are mostly girls, suddenly began identifying with Trans after spending a lot of time online and or with friends who became Trans.
In 2023, a study was published of 1,655 parent reports of Rapid Onset Gender Dysphoria. Here is a link to this study:
https://www.researchgate.net/publication/375734946
Here are quotes:
During the past decade there has been a dramatic increase in adolescents and young adults (AYAs) complaining of gender dysphoria. One explanation is that the increase reflects a socially contagious syndrome among emotionally vulnerable youth: rapid-onset gender dysphoria (ROGD). Advocates of the ROGD theory view the dramatic increase in referrals to gender clinics with alarm. They are concerned that adolescents with ROGD are at risk of unnecessary, harmful, and irreversible psychological and medical interventions.
Some of these groups are quite large, with Gender Critical Support Board exceeding 3,500 registered members, and Parents of Transgender Children exceeding 8,000 members. (Both numbers taken from their respective websites on April 12, 2022.
We report results from a survey of parents who contacted the website ParentsofROGDKids.com because they believed their AYA children had ROGD. Results focused on parent reports on 1,655 AYA children whose gender dysphoria began between ages 11 and 21 years, inclusive. These youths were disproportionately (75%) natal female. Natal males had later onset (by 1.9 years) than females, and they were much less likely to have taken steps towards social gender transition (65.7% for females versus 28.6% for males). Pre-existing mental health issues were common, and youths with mental health issues were more likely than those without them to have socially and medically transitioned. Parents reported that they had often felt pressured by clinicians to affirm their AYA child’s new gender and support their transition. According to the parents, AYA children’s mental health deteriorated considerably after social transition.
21 Florida judge rules gender mutilation is safe and effective
In the first section of this report, we quoted an August 21, 2023 decision by a three judge panel who agreed that Alabama has a rational basis for banning gender mutilation of minors in their state. The case was called Eknes-Tucker v. Governor, State of Alabama.
Sadly, on June 11, 2024, a single federal judge in Florida named Robert Hinkle ignored this three judge Alabama decision and ruled that Florida did not have a rational basis for banning gender mutilation of minors in their state.
https://storage.courtlistener.com/recap/gov.uscourts.flnd.460963/gov.uscourts.flnd.460963.223.0.pdf
Republican Gov. Ron DeSantis’ office blasted Hinkle’s ruling, issuing a statement calling it “erroneous,” and vowing to appeal.
“Through their elected representatives, the people of Florida acted to protect children in this state, and the Court was wrong to override their wishes,” the statement said. “As we’ve seen here in Florida, the United Kingdom, and across Europe, there is no quality evidence to support the chemical and physical mutilation of children. These procedures do permanent, life-altering damage to children, and history will look back on this fad in horror.”
The Florida judge dismissed the statements of all of the state’s witnesses by claiming without any supporting evidence that anyone opposed to gender mutilation must be an irrational religious zealot who was misled by their religious biases into discriminating against a trans child. The judge appeared to be completely unaware of underlying mental health problems or that more than 90% of such children no longer wanted to change their gender once they grew up. The judge also seemed to be completely unaware that Sweden changed course on drugging children after long term studies found extreme harm to these children. Clearly, the leaders of Sweden are not irrational religious zealots.
At the same time, the judge blindly accepted - again without evidence - that the supporters of gender mutilation represented the accepted opinion of the medical community.
The judge also accepted the claim that giving kids drugs and subjecting them to surgeries was safe and effective – never bothering to read the actual studies that concluded that the drugs and surgeries were not safe or effective.
Instead, the judge accepted the claims of drug pushers as as if gender mutilation was no more harmful to a child than giving the disturbed child a free trip to Disneyland. The judge repeatedly used the misleading term “gender-affirming care” as if gender mutilation and experimental drug interventions had not a single adverse consequence.
The truth will hopefully eventually come out that gender mutilation is indeed harmful to children as we get more long term scientific evidence of the results of this grotesque experiment on our children
22 King County Judge Rules against Parental Notification
On June 24, 2024, King County Judge Michael Scott issued an Injunction blocking the Parental Notice section of the Washington State Parental Rights Act – also known as Initiative 2081. Judge Scott, who was appointed to the court by Jay Inslee in 2018, ruled:
“Washington State shall cease all implementation and enforcement of Initiative 2081’s portions related to the time in which schools must provide records, including the requirement that parents “receive a copy of their child’s records within 10 business days of submitting a written request;” and Initiative 2081 to the extent that it requires disclosure of medical, health, and mental health records and/or information protected by RCW 70.02.020.”
This judge explained verbally that he was concerned about the 10 day notice because the federal law allows 45 days for educational records. What the judge failed to mention is that states are allowed to have health and education laws that are more strict than federal laws. For example, the law that Senate Bill 5599 amended (and that the Parents Rights Act is clarifying) requires parental notice in a maximum of 3 days. So the concern raised by the judge about 10 days notice is simply absurd.
In addition, there is not a single word in RCW 70.02.020 that prevents health care records of minors from being disclosed to their parents. So there are no records of minors that need to be protected from parents in RCW 70.02.020. Again, the judge’s reasoning for the Injunction is simply absurd.
But while it may be absurd, the Injunction will have devastating consequences for tens of thousands of parents and children here in Washington state. The injunction against parental notice of medical and mental health records will now stay in effect throughout the rest of the legal proceedings. These proceedings could take months or even years while the issue works its way through trial and appeals.
The injunction blocks important God-given parental rights that have existed throughout human history. Yet this judge has placed his opinion above the wishes of nearly a half million voters who signed the Initiative, and more than 10,000 voters who committed on the bill during legislative hearings – and above the opinion of a 49 to 0 vote in the Senate and an 80 to 14 vote in the House – with absolutely not even a hint during any of the Hearings – or a single claim by a single legislator – that the bill might not comply with either existing state law or our state constitution.
Equally bad, the injunction will likely stay in effect until the 2025 legislative session – at which time corrupt legislators are likely to strip Parental Notice from the Parents Rights Act – rendering the act meaningless. Two years of work by thousands of people to get Parents Rights in Washington State will have gone down the drain.
But worst of all is the fact that this judge’s ruling will keep hidden from parents child mutilation crimes currently being committed against their children – child mutilation procedures that are based on lies and not supported by any science and are certain to cause a lifetime of harm for their victims, lies and harms.
Finally, this injunction will keep these crimes hidden from the voters through the remainder of the 2024 election. This is something we must not let happen. It is now up to all parents and grandparents to make Parents Rights an election issue in the 2024 election.
Verbal comments by Judge Scott
In his verbal decision to grant the preliminary injunction against the Parents Rights Act, Scott raised concerns over the language in the initiative calling for schools to turn over all medical and mental health records and to do so within 10 days of a parents request. He noted that the federal Family Educational Rights and Privacy Act (FERPA) requires schools to turn over records as soon as possible, or within 45 days of the request.
The opponents of the Parents Rights Initiative claim in their lawsuit that existing Washington law (Senate Bill 5599 passed in 2023) gave minors in Washington the right to hide experimental and life-harming drug doses – administered while they are in school - from their parents. However, the actual wording in the Parents Rights Act does not contradict the child’s right to be given these drugs. It merely requires that parents be notified about the life-harming drugs before the drugs are given to the child. With the Injunction, parents will continue to be kept in the dark.
23 Supreme Court to review state bans on gender mutilation of minors
On June 24, 2024, the US Supreme Court announced that they will review state bans on gender-affirming care for minors (more accurately called gender mutilation of minors) during their Fall session in October. The court will consider the constitutionality of state laws that restrict or ban gender-mutilation of minors, including hormone therapy and surgeries.
The specific case they will review involves a Tennessee law that prohibits healthcare providers from administering puberty blockers, hormones, and surgeries to minors. The law was challenged by the Biden administration, who argue that it violates the equal protection clause of the 14th Amendment and the due process clause of the 14th Amendment as well as a 2020 US Supreme Court decision called Bostock v. Clayton County.
While the lower court had applied the Supreme Court’s 2020 decision...to equate “gender identity” with “sex” as used in Title VII, the 6th Circuit Court of Appeals disagreed concluding that the Supreme Court 2020 decision was limited to job discrimination of adults and therefore did not apply to gender mutilation via giving experimental drugs to minors. In a two to one vote on July 8, 2023, the 6th Circuit held that the Tennessee state law did not violate either parents’ constitutional right to direct the upbringing of their children or constitutional protections that require all individuals to be treated equally regardless of sex. Here is a link to the 6th Circuit ruling: https://www.opn.ca6.uscourts.gov/opinions.pdf/23a0146p-06.pdf
Here is a quote from their decision:
“Parents, it is true, have a substantive due process right “to make decisions concerning the care, custody, and control of their children.” Troxel v. Granville, 530 U.S. 57, 66 (2000). But the Supreme Court cases recognizing this right confine it to narrow fields, such as education, Meyer v. Nebraska, 262 U.S. 390 (1923), and visitation rights, Troxel, 530 U.S. 57. No Supreme Court case extends it to a general right to receive new medical or experimental drug treatments.“
The above Court of Appeals ruling caused a Kentucky Federal court to rule in favor of Kentucky ban on gender mutilation of minors.
On August 21, 2023, the 11th Circuit Court of Appeals issued a similar opinion, voting three to zero in favor of a similar Alabama state ban.
Here is a link to their 59 page opinion.
https://media.ca11.uscourts.gov/opinions/pub/files/202211707.pdf
Here is a quote: “States have a compelling interest in protecting children from drugs, particularly those for which there is uncertainty regarding benefits, recent surges in use, and irreversible effects… these medications can cause loss of fertility and sexual function.”
In a similar ruling, on August 25, 2023, a federal court upheld the constitutionality of a Missouri law banning giving gender mutilation drugs to minors. Here is a link to this ruling: https://ago.mo.gov/wp-content/uploads/sb-49-order.pdf?sfvrsn=1a3d0aea_2
In February, 2024, a three judge panel of the 7th Circuit of the Court of Appeals also held for the state of Indiana ban. They said they would issue an opinion at some point in the future but as of June 2024, they have not issued an opinion – just a decision.
On November 16, 2022, in a 6 to 5 decision, the 8th Circuit has blocked a gender affirming care ban in Arkansas.
https://fingfx.thomsonreuters.com/gfx/legaldocs/byprljlzrpe/Brandt%20v%20Rutledge%20en%20banc%20denial%2011-16.pdf
In December 2023, a 9th Circuit three judge panel blocked a gender affirming care ban in Idaho. However, on April 15, 2024, the US Supreme Court by a vote of 6 to 3 granted Idaho Attorney General Raúl Labrador’s (R) request to narrow a December district court order blocking the state’s ban in its entirety, allowing the law to be enforced against individuals other than the two transgender teenagers challenging it in court.
As we noted earlier in this report, a court in Texas ruled in favor of the state ban while a court in Florida ruled against the state ban. There are at least 7 more federal courts that may issue opinions before the Supreme Court hears the case in October. But so far, there are about 12 federal judges ruling for State bans and 5 federal judges ruling against state bans. In addition, there are about 27 state attorney generals in favor of state bans and 16 attorney generals (including the Washington state attorney general) who have submitted briefs opposing the state bans.
My prediction is that the US Supreme Court will rule 6 to 3 that the 2020 US Supreme Court decision called Bostock v. Clayton County does not apply to gender mutilation bans of minors.
A ruling in favor of the states will allow them to continue restricting or banning gender mutilation of minors, which will likely lead to a patchwork of state by state laws across the US. As voters learn more about how “gender-affirming drugs” have serious adverse consequences, they will vote against the corrupt politicians who support this drug abuse and vote in favor of politicians who support protecting minors from gender mutilation drug peddlers.
Hopefully, some day the truth will come out and those who committed this crime against our kids will be held accountable for the lies they told and the damage they inflicted on our children.
24 Resolution Opposing School Clinics Giving Gender Mutilation Drugs to Minors
Whereas School based health clinics (SBHCs) are tax payer funded medical clinics placed inside of schools in order to give gender mutilation drugs to minors without the consent or knowledge of their parents, and
Whereas the number of School Based Health Centers (SBHCs) in Washington State has more than doubled from under 30 in 2019 to more than 70 in 2024 – now located in more than 30 school districts, and
Whereas long-standing State and federal parental notification laws are bypassed because the employees of the SBHC are not technically employees of the school district, and
Whereas the danger of SBHCs is that parents and students can be misled into thinking that the SBHC is a part of the school when it is in fact a separate business, and
Whereas parents may not know that students can receive experimental and even dangerous gender mutilation drugs at an SBHC without parents knowledge or consent, and
Whereas advocates of Gender Mutilation drugs (also called Gender Affirming Care) claim that giving kids gender drugs saves lives and reduces the suicide rate when fact, giving kids gender drugs is known to cost lives and increase the suicide rate, and
Whereas advocates of SBHCs claim they lower health care costs when in fact SBHCs have dramatically increased health care costs for minors as dangerous gender mutilation drugs can cost hundreds of thousands of dollars per child, and
Whereas more than 25 states and several nations have banned giving gender mutilation drugs to minors.
Therefore, be it resolved that we oppose locating SBHCs in schools here in Washington State and we ask our state legislature to join other states in passing a law banning giving minors gender mutilation drugs.
Organization: _______________________ Date: _____________
For additional information, visit Washington Parents Network.com
25 Four Steps to protect our kids from state child abuse
Forcing Kindergartners to use gender pronouns that do not match the biological sex of a person is more than just confusing. It is child abuse in that it is the first step that might send a vulnerable child down an extremely dark path. Even worse, telling children that they should not trust their parents and that they should even lie to their parents is certain to damage their essential relationship with their parent. It is time to end the abuse of our children! Truth is power and it is time to expose the lies Reykdal has been telling us about what is happening in our public schools.
Our first goal is to replace Chris Reykdal with a State Superintendent who understands the importance of parents rights. Our second goal is to elect State legislators who pledge to support parents rights and local control of our schools. Our third goal is to elect and support School Board Directors who support parents rights and local control of our schools.
If you agree that it is time to build a political movement capable of winning elections so we can replace Chris Reykdal and the current anti-parent legislature, then please consider taking one or more of the following steps:
Step #1: Sign up for our newsletter to get once a week updates on our coming events.
Step #2: Help spread the word by sharing this website with other parents, grandparents, school board members and concerned citizens. Our goal is to organize parents in every school district in Washington state.
Step #3: Attend one or more of our weekly statewide online video conference organizing meetings – which at least initially will be held on Sundays from 3 to 4 pm beginning Sunday June 16 (which is also Fathers Day). The purpose of these meetings will be to meet and build relationships with others in our state who want to take action on restoring parents rights and protecting our children from state-sponsored child abuse. Our goal is to grow our weekly video conference meetings large enough to add regional or county meetings from 4 to 5 pm and eventually have legislative district meetings from 5 to 6 pm and school district meetings from 6 to 7 pm.
For a link to our next online meeting, send an email to David at Washington Parents Network dot com with your name and the county you live in.
Step #4: Organize a Washington Parents Network meeting in your community to help educate and organize local parents to end this horrible abuse of our kids. We will be traveling around Washington state to answer questions about this danger and to train local leaders on why and how to restore parents rights to raise their children. If you are a member of a county organization, legislative district organization, church or local community group, send us an email and we will find a date and time to arrange an in-person meeting with your group. As always, I look forward to your questions and comments – and I look forward to meeting you!
Regards,
David Spring M. Ed.
David at Washington Parents Network dot com